
Urology — MCQs

On this page
All are true about the conditions shown in the figure except?

The following instrument is used for:

Which is incorrect about the swelling shown below?

Identify the instrument shown in the image:

Which is incorrect about the procedure shown in the patient with right flank pain?

What does the following image show?

During evaluation of a child with recurrent UTI, VCUG is performed and the following finding is observed. What is the diagnosis?

The radiographic image shows a stent in the urinary tract. This type of stenting is most commonly performed following which procedure?

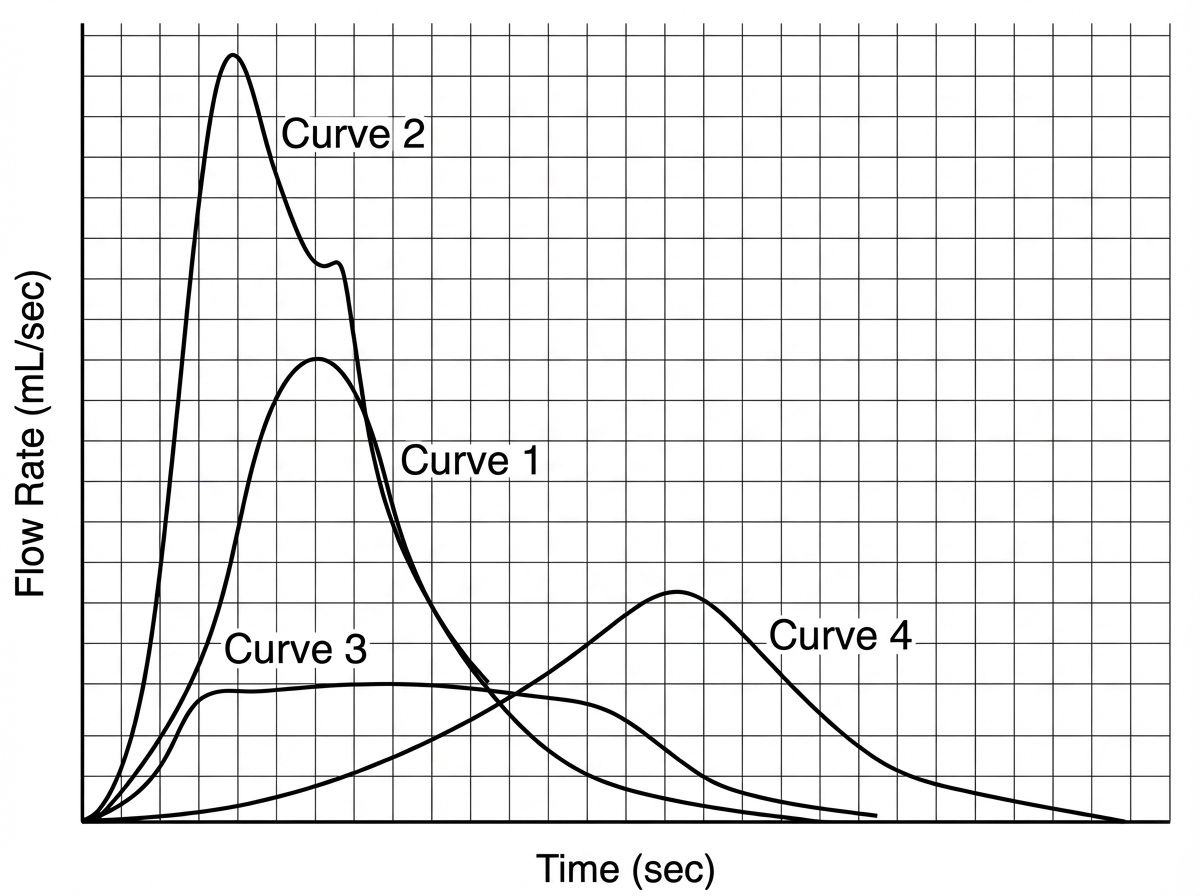
Which of the following uroflowmetry recording indicates BPH?
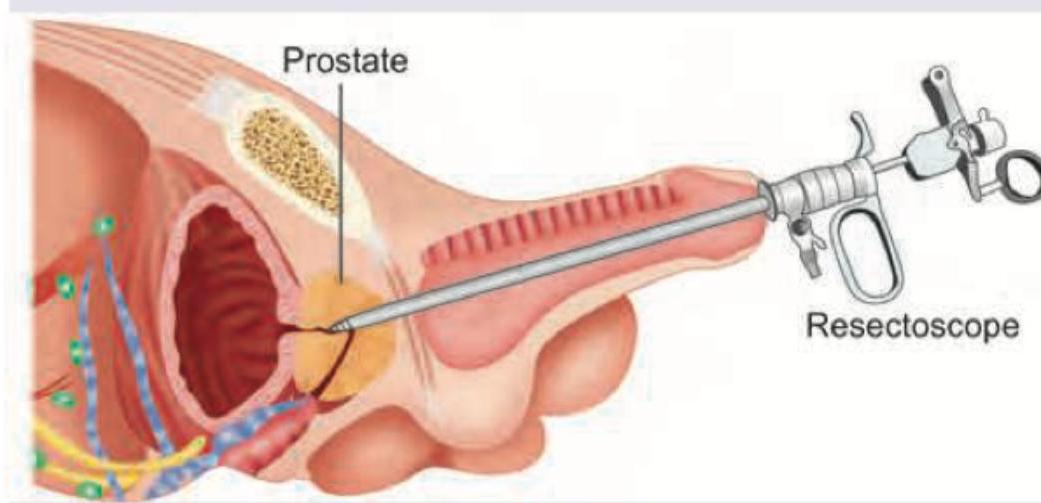
A 70-year-old man underwent the procedure shown below. 3rd day he develops seizures. What is the diagnosis?
Practice by Chapter
Urological Anatomy
Practice Questions
Hematuria Evaluation
Practice Questions
Urinary Calculi
Practice Questions
Benign Prostatic Hyperplasia
Practice Questions
Prostate Cancer
Practice Questions
Bladder Cancer
Practice Questions
Renal Cell Carcinoma
Practice Questions
Testicular Tumors
Practice Questions
Urinary Tract Infections
Practice Questions
Urinary Incontinence
Practice Questions
Genitourinary Trauma
Practice Questions
Pediatric Urology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app