
Urology — MCQs

On this page
What is a potential complication of performing percutaneous nephrolithotomy (PCNL) through the 11th intercostal space?
Most common presentation of renal cell carcinoma is
A 27-year-old man presents with a left testicular tumor and a 10 cm retroperitoneal lymph node mass. Which of the following is the treatment of choice?
Which of the following statements about Varicocele is false?
In which of the following conditions is circumcision specifically indicated?
A 60-year-old smoker presented with a history of a single episode of painless gross hematuria. The most logical investigation would be.
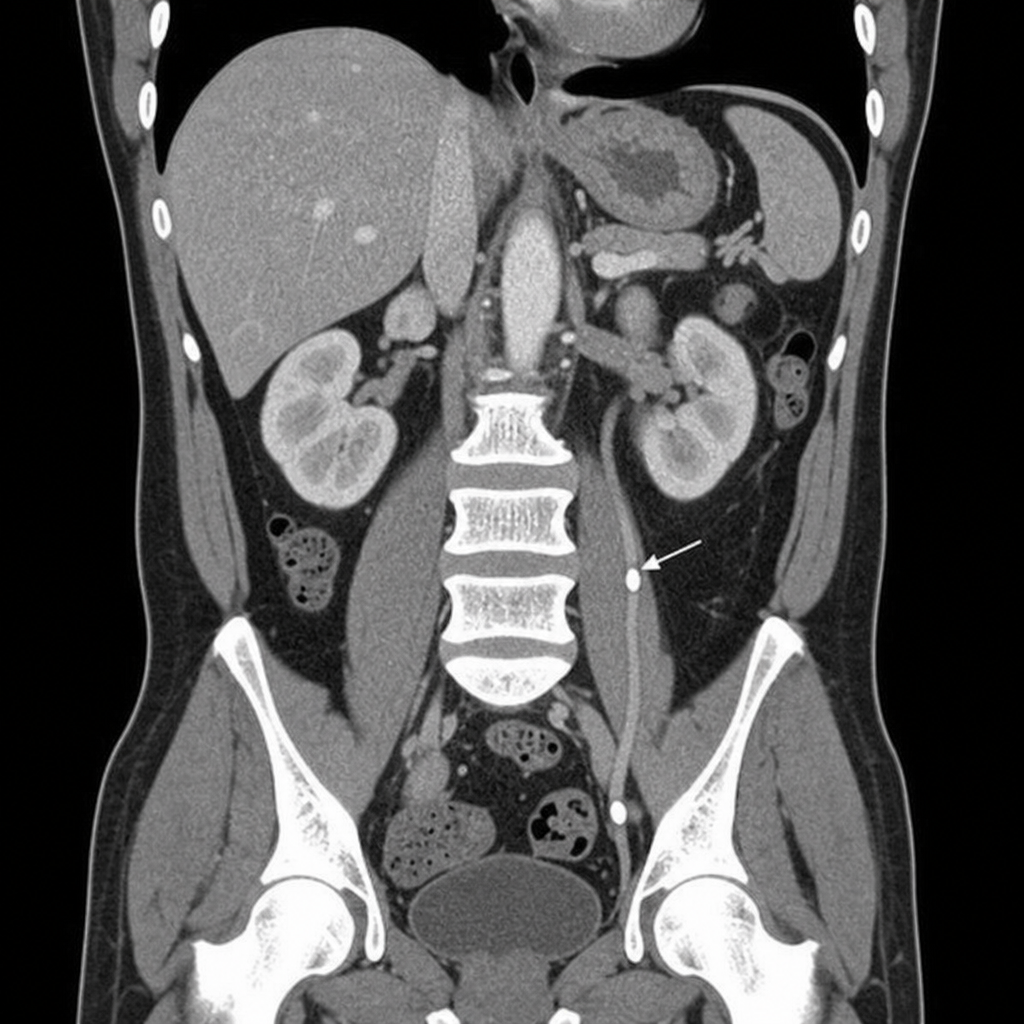
A 40-year-old male presented to the casualty with severe pain in the left upper abdomen radiating to the groin. Urine routine examination shows 6-8 pus cells and 15-20 red blood cells. What is the diagnosis based on the CT scan findings?
What is the most common type of stone found in the bladder?
During TURP, the surgeon takes care to dissect above the verumontanum to avoid injury to
Which of the following is NOT a suitable management option for accidental injury of the ureter during an abdominal operation?
Practice by Chapter
Urological Anatomy
Practice Questions
Hematuria Evaluation
Practice Questions
Urinary Calculi
Practice Questions
Benign Prostatic Hyperplasia
Practice Questions
Prostate Cancer
Practice Questions
Bladder Cancer
Practice Questions
Renal Cell Carcinoma
Practice Questions
Testicular Tumors
Practice Questions
Urinary Tract Infections
Practice Questions
Urinary Incontinence
Practice Questions
Genitourinary Trauma
Practice Questions
Pediatric Urology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app