
Urology — MCQs

On this page
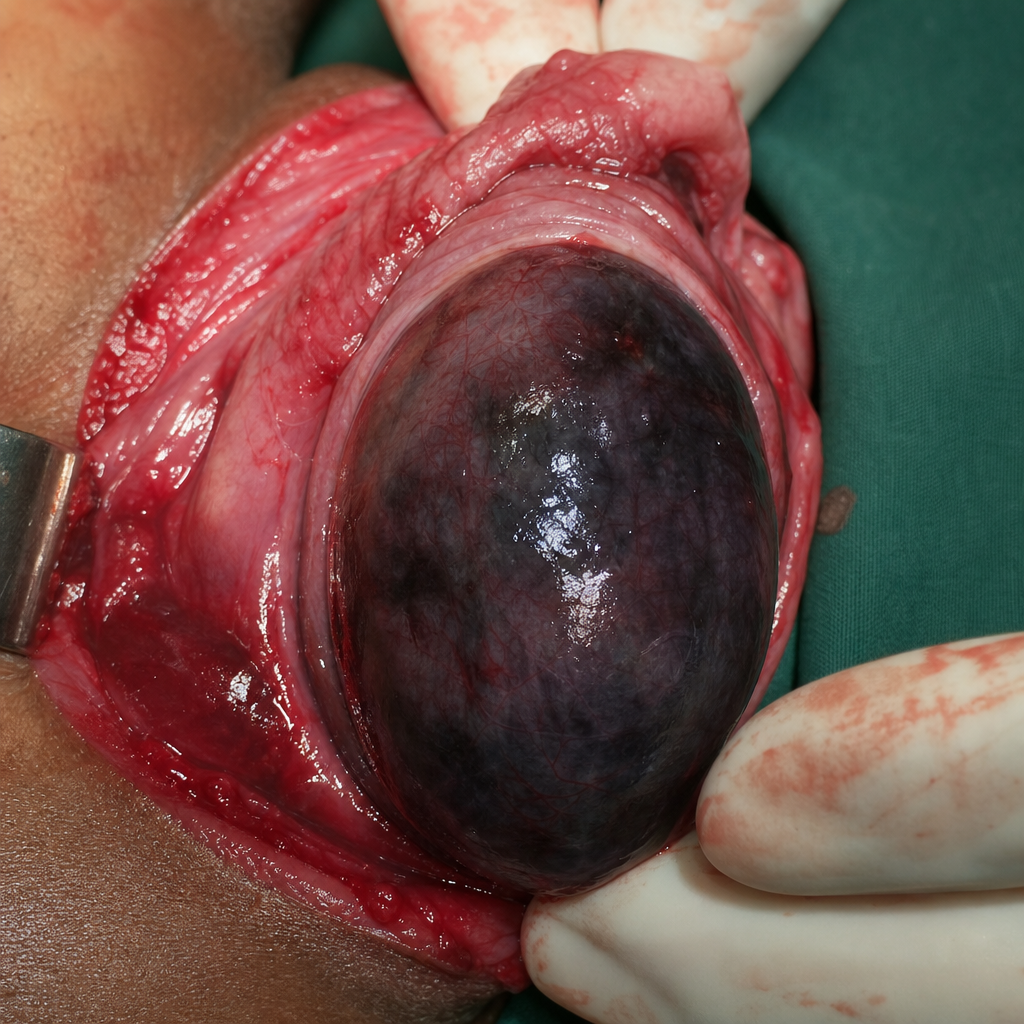
A 12-year-old child presents to the OPD with a complaint of scrotal pain and a history of trauma 6 hours ago. Doppler ultrasound shows absent blood flow to the testis. On surgical exploration, a twisted spermatic cord is identified and the following finding is observed. What is the most likely diagnosis?
An 85-year-old male with prostate cancer, Gleason score of 6 , and PSA <8 ng/mL. What is the best management approach?
A 30-year-old male undergoes varicocele surgery to correct his left-sided varicocele. Following the procedure, the surgeon explains the postoperative changes to the patient. The patient asks, "Through which route does the venous drainage primarily occur after the surgery?" Which of the following is the correct response by the surgeon?
A 50 year old male patient came to the outpatient department with complaints of hematuria. A 2 x 2 cm bladder mass is seen which is low grade transitional cell carcinoma. Which among the following is the ideal management?
The complication which will not occur after PCNL surgery:
Which of these is the best for management of a 3 cm stone in renal pelvis without evidence of hydronephrosis?
Prostatic cancer mostly seen in
A 62-year-old female had a kidney stone and was treated with PCNL. After 2 days, she comes to the OPD with chills and fever. What is the complication?
Bell clapper deformity (abnormal testicular fixation) predisposes to which of the following conditions?
Time cut-off for diagnosis of Priapism is?
Practice by Chapter
Urological Anatomy
Practice Questions
Hematuria Evaluation
Practice Questions
Urinary Calculi
Practice Questions
Benign Prostatic Hyperplasia
Practice Questions
Prostate Cancer
Practice Questions
Bladder Cancer
Practice Questions
Renal Cell Carcinoma
Practice Questions
Testicular Tumors
Practice Questions
Urinary Tract Infections
Practice Questions
Urinary Incontinence
Practice Questions
Genitourinary Trauma
Practice Questions
Pediatric Urology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app