
Urology — MCQs

On this page
Which of the following are correct about ectopic ureters? 1. They are more common in males 2. They drain the upper pole of the kidney 3. They are associated with duplex ureter 4. They may cause incontinence
The following operative procedure can result in neurogenic voiding dysfunction except:
Indications of TURP for Benign Prostatic Hyperplasia (BPH) include: 1. Urinary flow rate of less than 10 mL/second 2. Residual volume of urine >100 mL 3. Serum level of prostatic specific antigen >10 ng/mL 4. Trabeculated Urinary bladder Select the correct answer using the code given below:
Hyperchloremic acidosis is a common complication of:
Urinary bladder can be injured in all of the following operations EXCEPT:
Intraoperative recognition of ureter is by which of the following features? 1. Transparent tubular appearance 2. Pale glistening appearance 3. Longitudinal vessels on surface 4. Circumferential vessels on surface Select the correct answer using the code given below:
A 22-year-old male rugby player presents with acute scrotal pain that began 2 hours ago. Physical examination shows a high-riding, tender left testis with an absent cremasteric reflex. Doppler ultrasound shows decreased blood flow to the left testis. What is the time-sensitive factor most critical to testicular salvage?
Which of the following statements is incorrect regarding vasectomy?
A patient presents with a penile lesion staged as T3, with clinically palpable lymph nodes. What is the most appropriate management?
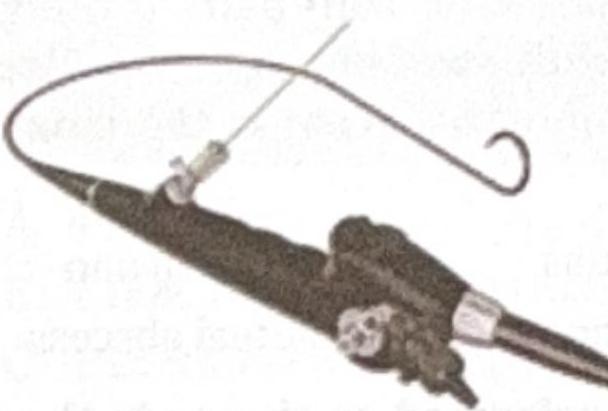
Identify the instrument shown in the image.
Practice by Chapter
Urological Anatomy
Practice Questions
Hematuria Evaluation
Practice Questions
Urinary Calculi
Practice Questions
Benign Prostatic Hyperplasia
Practice Questions
Prostate Cancer
Practice Questions
Bladder Cancer
Practice Questions
Renal Cell Carcinoma
Practice Questions
Testicular Tumors
Practice Questions
Urinary Tract Infections
Practice Questions
Urinary Incontinence
Practice Questions
Genitourinary Trauma
Practice Questions
Pediatric Urology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app