
Urology — MCQs

On this page
A 65-year-old patient presents with sudden pain in the scrotum associated with prostration, pallor and pyrexia. What could be the most probable diagnosis?

All are true about the conditions shown in the figure except?

The following instrument is used for:

What is the most likely diagnosis based on the clinical image?

Which is incorrect about the swelling shown below?

Which is incorrect about Extracorporeal Shockwave Lithotripsy (ESWL) in the management of the patient with right flank pain shown in the image?

A patient underwent pyeloplasty. The following radiograph was obtained postoperatively. What does the image show?

During evaluation of a male child with recurrent UTI, VCUG is performed and the following finding is observed. What is the diagnosis?

The radiographic image shows a double-J stent in the urinary tract. Which procedure routinely uses a double-J stent to splint a ureteropelvic anastomosis?

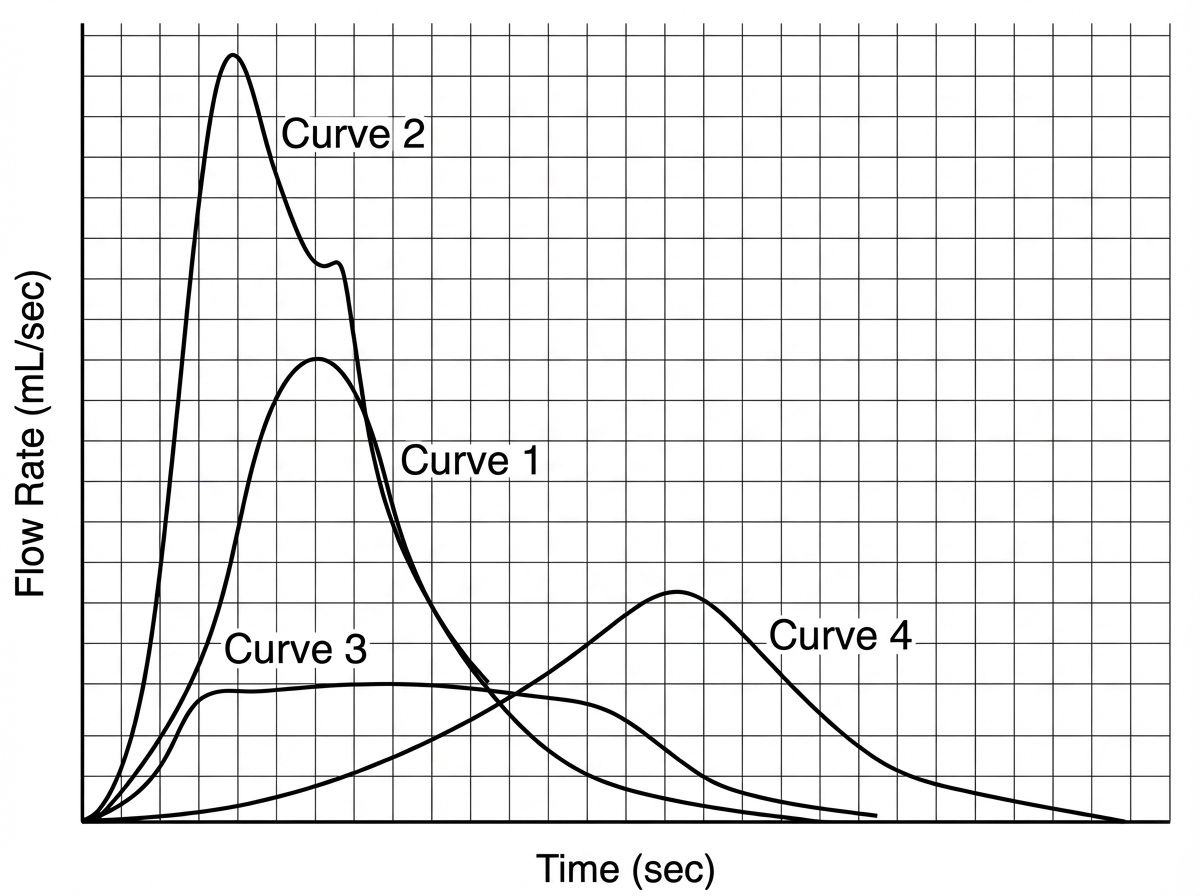
Which of the following uroflowmetry recording indicates bladder outlet obstruction?
Practice by Chapter
Urological Anatomy
Practice Questions
Hematuria Evaluation
Practice Questions
Urinary Calculi
Practice Questions
Benign Prostatic Hyperplasia
Practice Questions
Prostate Cancer
Practice Questions
Bladder Cancer
Practice Questions
Renal Cell Carcinoma
Practice Questions
Testicular Tumors
Practice Questions
Urinary Tract Infections
Practice Questions
Urinary Incontinence
Practice Questions
Genitourinary Trauma
Practice Questions
Pediatric Urology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app