
Urology — MCQs

On this page
A patient presents with urinary symptoms due to benign prostatic hyperplasia. Which of the following is used to manage the urinary symptoms in the initial stage of this condition?
A 60-year-old patient presents with painless hematuria. He is diagnosed with bladder cancer involving the muscle layer. What is the next best step in the treatment of this patient?
Which of the following will have unilateral hydronephrosis?
A 44-year-old lady presents to the hospital with a ballotable flank mass. On CT imaging, the mass measures 4cm and is located in the renal cortex, with no involvement of the renal pelvis or collecting system, making upper-tract urothelial carcinoma unlikely. What is the most appropriate management for her condition?
How long should a couple use contraception post-vasectomy?
A 35-year-old patient presents with colicky pain and is diagnosed with a ureteric stone. Which of the following is the best diagnostic investigation in this case?
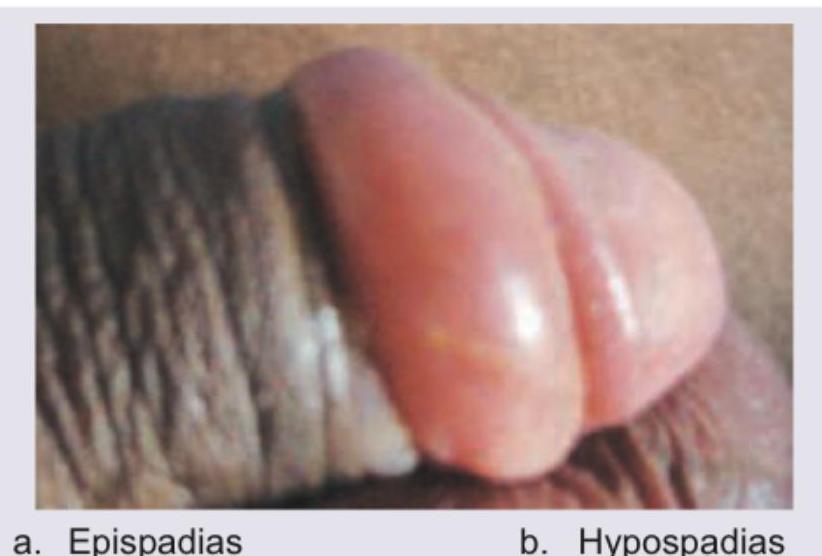
What is incorrect about the image shown?

What is the clinical diagnosis?
An 18-year-old patient presents with sudden agonizing pain in the groin and the lower abdomen. On physical examination, the testis seems high. The cremasteric reflex is lost. What is the most possible cause?
A 24-year-old male patient complains of painful and involuntary erection. Which of the following statement is false regarding this patient?

Practice by Chapter
Urological Anatomy
Practice Questions
Hematuria Evaluation
Practice Questions
Urinary Calculi
Practice Questions
Benign Prostatic Hyperplasia
Practice Questions
Prostate Cancer
Practice Questions
Bladder Cancer
Practice Questions
Renal Cell Carcinoma
Practice Questions
Testicular Tumors
Practice Questions
Urinary Tract Infections
Practice Questions
Urinary Incontinence
Practice Questions
Genitourinary Trauma
Practice Questions
Pediatric Urology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app