
Urology — MCQs

On this page
A 50-year-old male presents with a hard scrotal swelling. Which of the following investigations is NOT indicated?
Which of the following statements about pyonephrosis is FALSE?
A 42-year-old paraplegic woman with a neurogenic bladder requires an indwelling urinary catheter. She develops a urinary tract infection and is seen by a urologist. Radiographic studies demonstrate a large stone that fills and follows the contours of the renal pelvis. The stone is most likely composed of which of the following?
Which of the following is a communicating hydrocele?
Which of the following is a common retroperitoneal tumor?
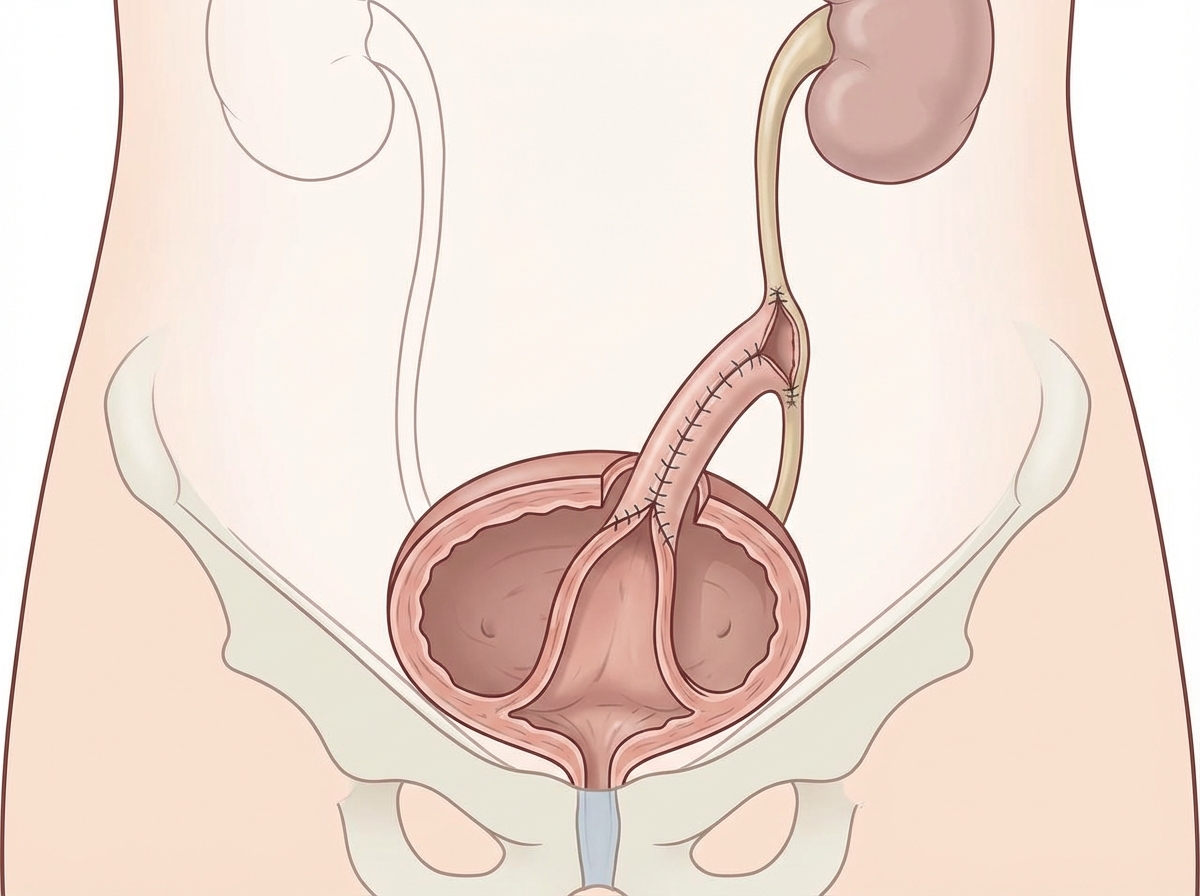
Name the operation shown here.
Which of the following statements regarding pain of renal and urinary tract origin is true?
What is the ideal method to remove a retained Foley's catheter if its balloon does not deflate?
During endoscopic surgery, what is the typical patient position?
Which of the following statements about vaginal hydrocele is false?
Practice by Chapter
Urological Anatomy
Practice Questions
Hematuria Evaluation
Practice Questions
Urinary Calculi
Practice Questions
Benign Prostatic Hyperplasia
Practice Questions
Prostate Cancer
Practice Questions
Bladder Cancer
Practice Questions
Renal Cell Carcinoma
Practice Questions
Testicular Tumors
Practice Questions
Urinary Tract Infections
Practice Questions
Urinary Incontinence
Practice Questions
Genitourinary Trauma
Practice Questions
Pediatric Urology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app