
Urology — MCQs

On this page
A young male presents with a scrotal swelling of 3 years duration. On examination, the swelling is fluctuant, and the testis is not separately felt. There is no history of trauma or fever. What is the most likely diagnosis?
Which of the following statements is true about seminoma?
According to the classification of renal injuries, which grade is assigned to a laceration more than 1 cm deep without extension into the renal pelvis or collecting system?
A 23-year-old male presented with fever, chills, and back pain. He also complained of increased frequency of voiding. Ultrasonography revealed bladder stones. All of the following are true about bladder stones, EXCEPT:
A male has a history of bilateral undescended testes. What is the most likely consequence?
The Hunt-Hess scale is used for the grading of which condition?
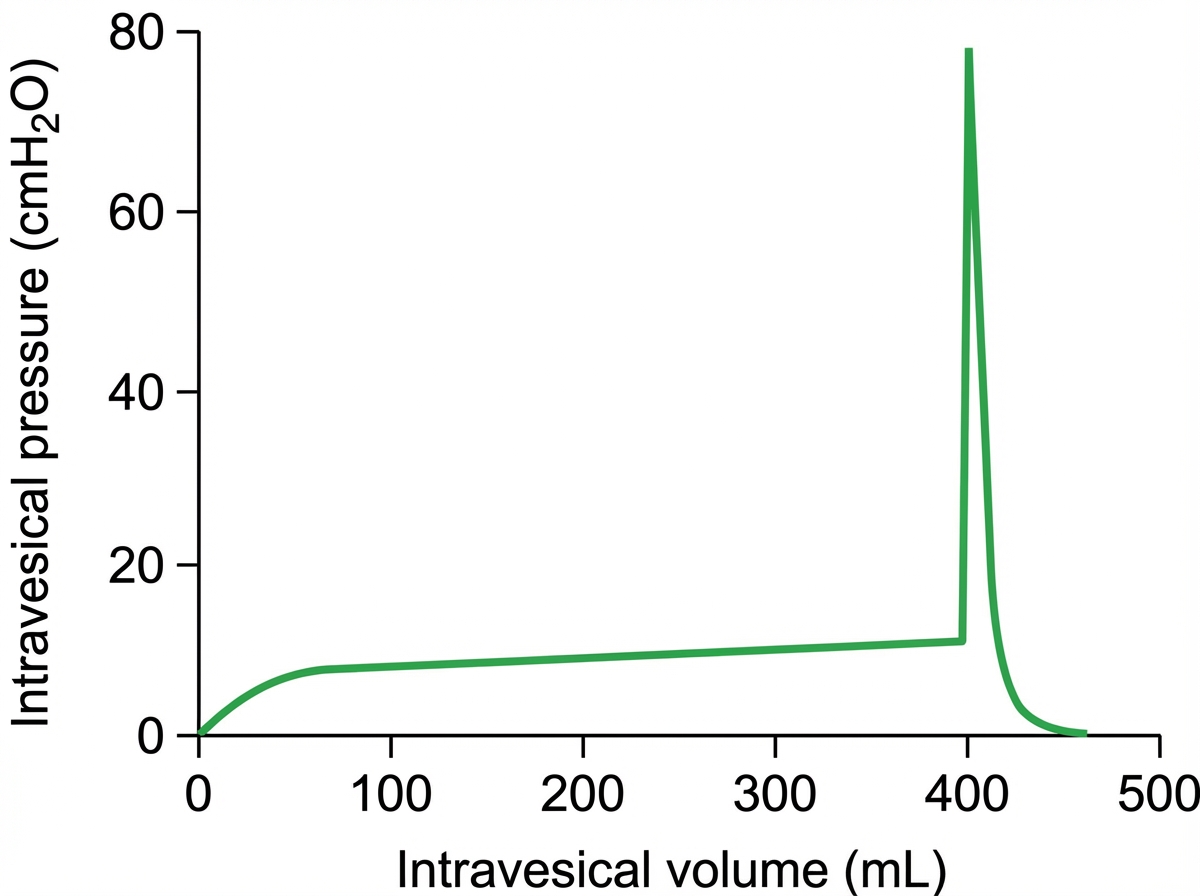
The graph shown in the illustration is known as:
What is the best treatment for Grade I benign prostate with outflow obstruction?
Which of the following is NOT a contraindication for extracorporeal shockwave lithotripsy for renal calculi?
All the following statements are true regarding torsion of testis EXCEPT?
Practice by Chapter
Urological Anatomy
Practice Questions
Hematuria Evaluation
Practice Questions
Urinary Calculi
Practice Questions
Benign Prostatic Hyperplasia
Practice Questions
Prostate Cancer
Practice Questions
Bladder Cancer
Practice Questions
Renal Cell Carcinoma
Practice Questions
Testicular Tumors
Practice Questions
Urinary Tract Infections
Practice Questions
Urinary Incontinence
Practice Questions
Genitourinary Trauma
Practice Questions
Pediatric Urology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app