
Urology — MCQs

On this page
What is the best treatment for meningioma with a low recurrence rate?
A 30-year-old male presents with a palpable mass related to the testis. On examination, the testis is enlarged and the mass is hard. What is the next best diagnostic step?
Antibodies against sperms may develop after which of the following procedures?
In renal transplant, where is the graft typically placed?
Hydrocele is a type of ……………… cyst?
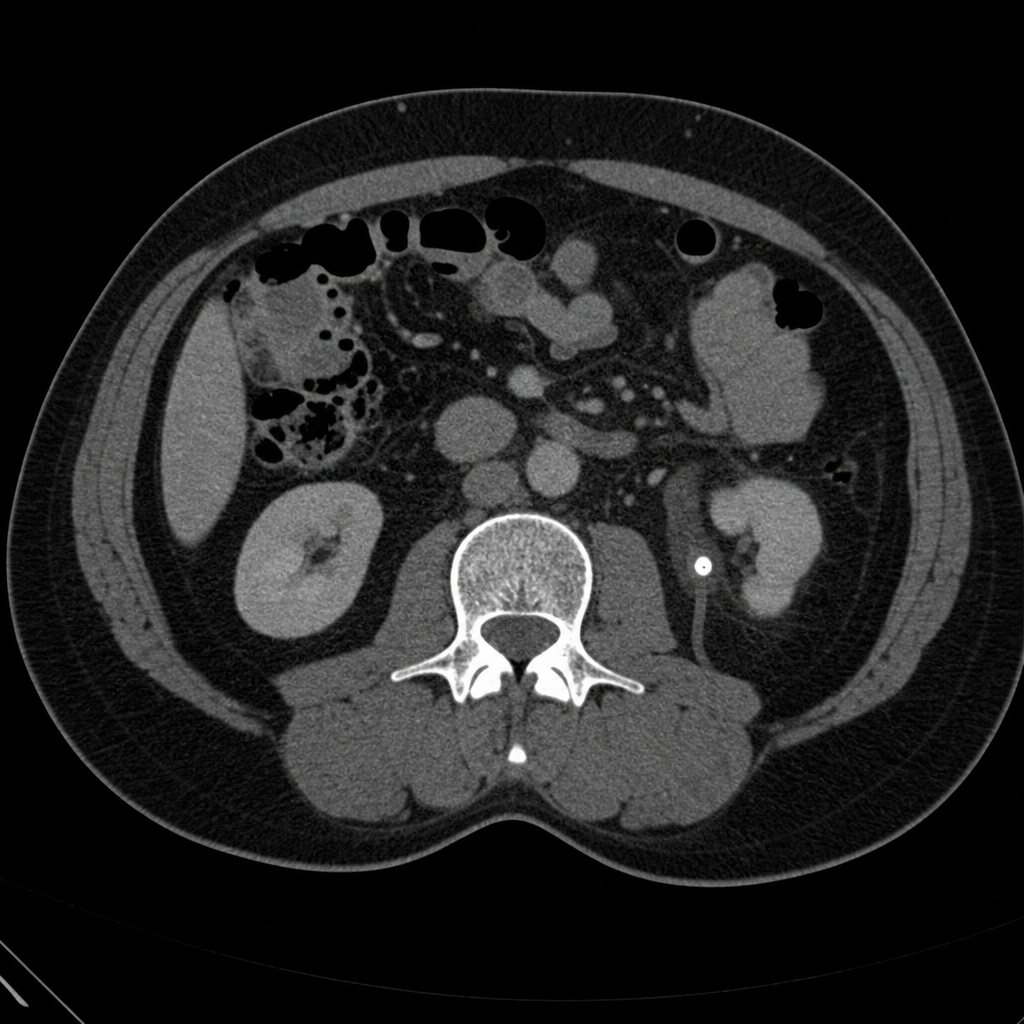
A 40-year-old male presents with severe left upper abdominal pain radiating to the groin. Urinalysis reveals 6-8 pus cells and 15-20 RBCs. A CT scan was performed. What is the most likely diagnosis?
Which of the following is a radio opaque stone?
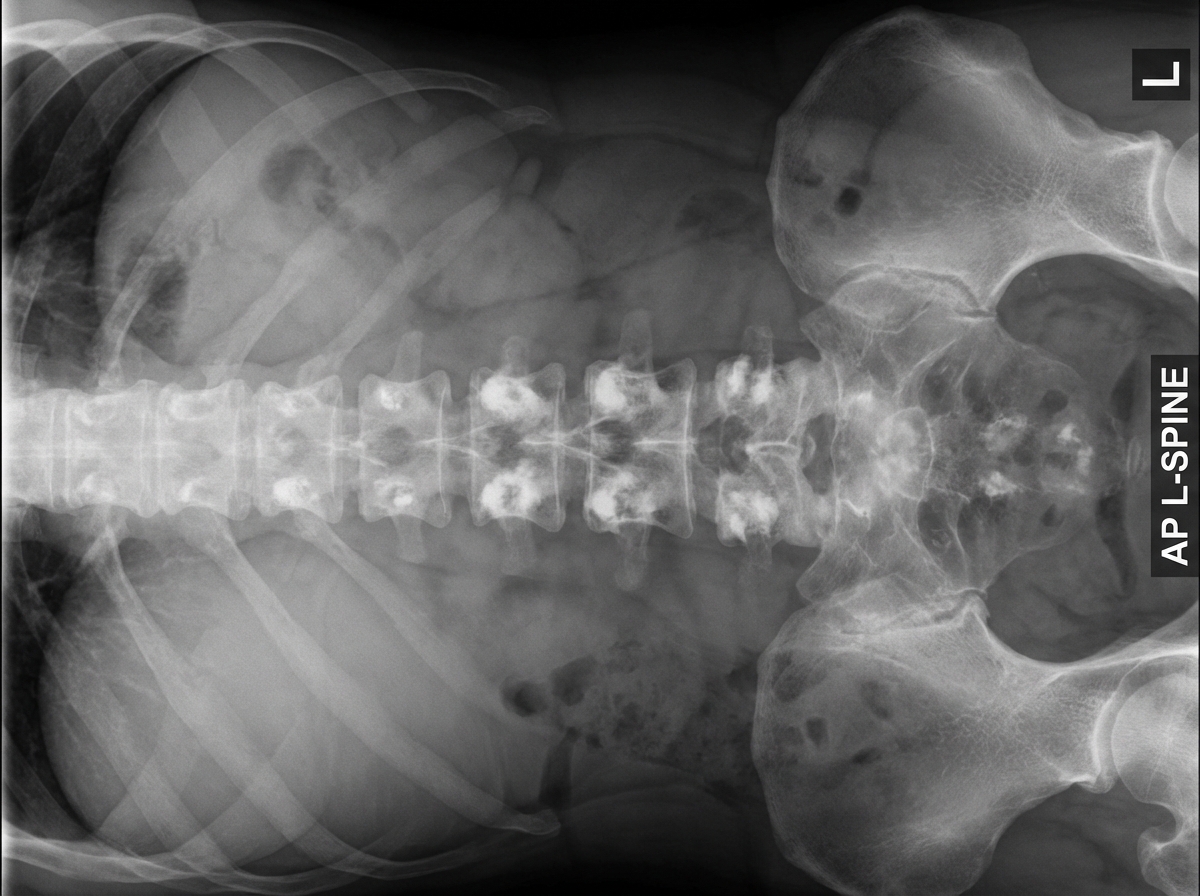
A 70-year-old male presents with signs of obstructive uropathy and severe, continuous pain in the back region. The provided X-ray of the patient's lumbar spine shows pathology. What is the most likely condition the patient is suffering from?
What percentage of testicular cancer is associated with cryptorchidism?
Which of the following is not a variant of PSA?
Practice by Chapter
Urological Anatomy
Practice Questions
Hematuria Evaluation
Practice Questions
Urinary Calculi
Practice Questions
Benign Prostatic Hyperplasia
Practice Questions
Prostate Cancer
Practice Questions
Bladder Cancer
Practice Questions
Renal Cell Carcinoma
Practice Questions
Testicular Tumors
Practice Questions
Urinary Tract Infections
Practice Questions
Urinary Incontinence
Practice Questions
Genitourinary Trauma
Practice Questions
Pediatric Urology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app