
Urology — MCQs

On this page
Which of the following conditions is characterized by a fluid-filled cyst that transilluminates and contains sperm-rich fluid?
A patient presents with persistent and severe pain in the lateral thigh and pubic regions, requiring hospital admission for observation and potential surgical intervention. Where is the ureteral stone most likely lodged?
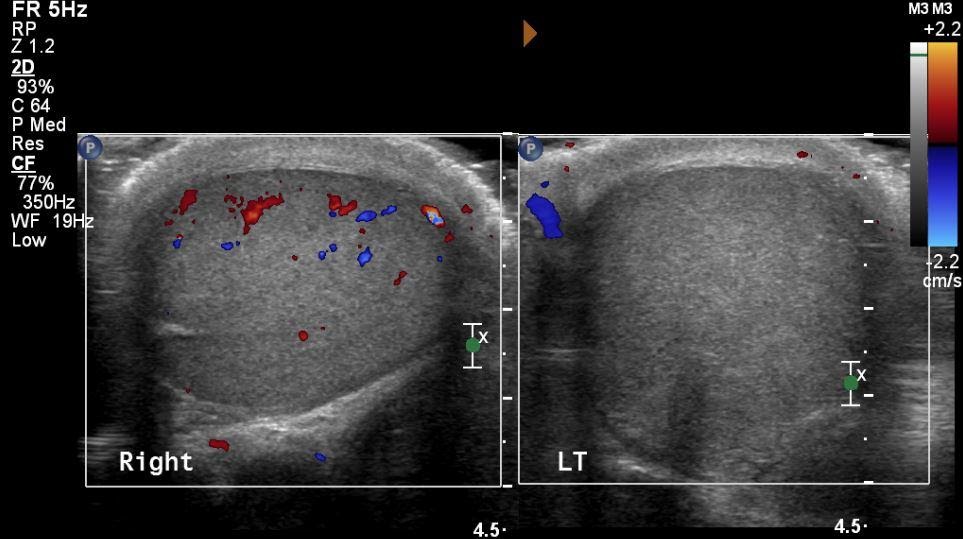
A 20-year-old male presented to the emergency department with acute onset of pain in the right scrotum. On examination, the testes were swollen, and the transillumination test was negative. What could be the probable diagnosis based on the ultrasound of the scrotum?
Which of the following structures in the spermatic cord is typically preserved (not divided) during vasectomy surgery?
Practice by Chapter
Urological Anatomy
Practice Questions
Hematuria Evaluation
Practice Questions
Urinary Calculi
Practice Questions
Benign Prostatic Hyperplasia
Practice Questions
Prostate Cancer
Practice Questions
Bladder Cancer
Practice Questions
Renal Cell Carcinoma
Practice Questions
Testicular Tumors
Practice Questions
Urinary Tract Infections
Practice Questions
Urinary Incontinence
Practice Questions
Genitourinary Trauma
Practice Questions
Pediatric Urology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app