
Trauma — MCQs

On this page
Which of the following investigations is/are true regarding rupture of the diaphragm?
What percentage of severe trauma is associated with extradural haematoma?
What is true regarding 'Damage control surgery'?
Trauma to spleen in a stable patient is best diagnosed by?
A patient with burns presents to the emergency room and has started on intravenous fluids. What is the best method to assess the adequacy of volume replacement?
A 26-year-old man is stabbed in the right intercostal space in the midclavicular line and presents to the emergency department. On examination, subcutaneous emphysema of the right chest wall, absent breath sounds, and a trachea shifted to the left are noted. What is the most likely serious diagnosis?
For the evaluation of blunt abdominal trauma, which of the following imaging modalities is ideal?
In a patient with a head injury, which of the following is most important to assess first?
What is considered a secondary brain injury?
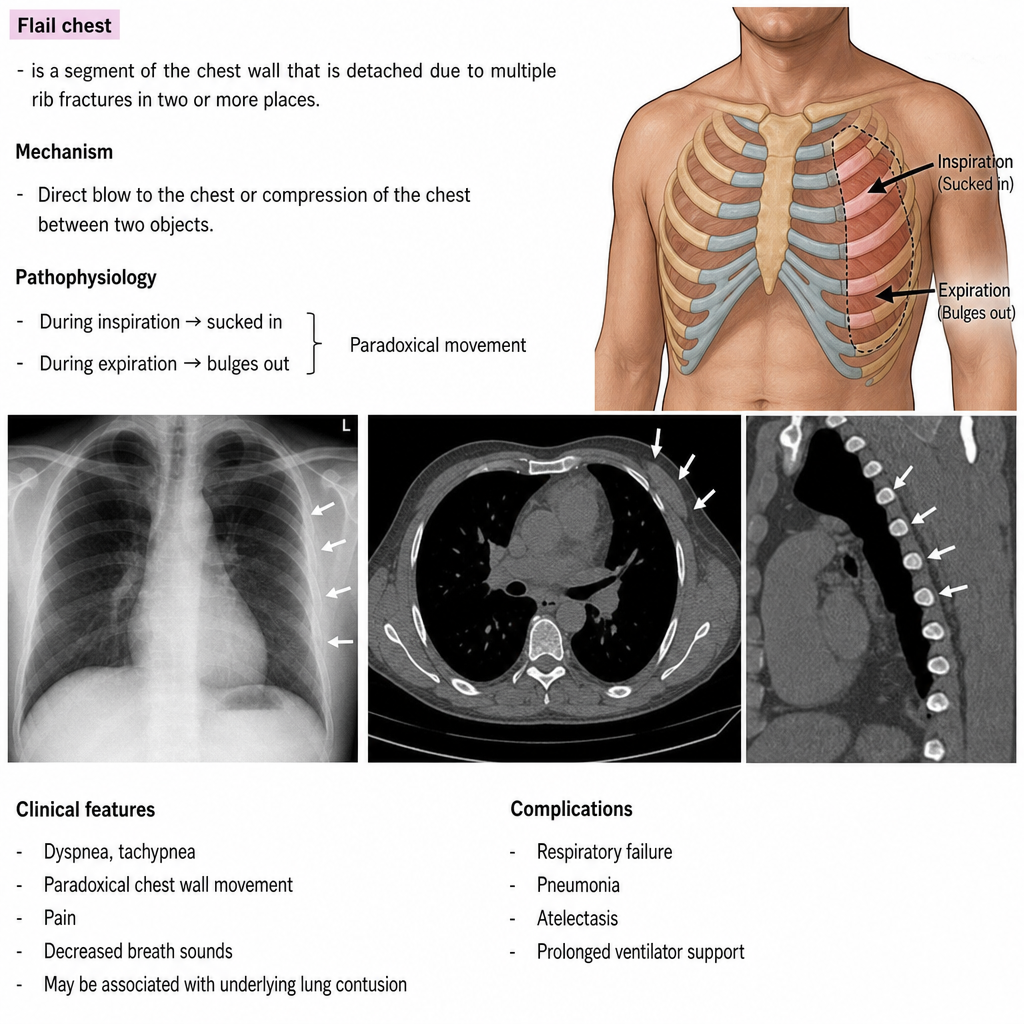
Which of the following statements are true about Flail chest? 1. Flail chest is characterized by paradoxical respiration of the affected chest wall segment. 2. The primary cause of hypoxia in flail chest is the paradoxical movement of the chest wall segment rather than underlying pulmonary contusion. 3. Every case of flail chest requires mechanical ventilation as the primary management. 4. Internal pneumatic stabilization using positive pressure ventilation helps stabilize the flail segment. 5. Surgical fixation of the ribs is indicated in patients who cannot be weaned from the ventilator or have severe chest wall deformity.
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app