
Trauma — MCQs

On this page
What is the treatment for class I hypovolemic shock?
Sign of basal skull fracture is all Except
A patient is brought to the emergency following a head-on collision road traffic accident. His BP is 90/60 mmHg. Tachycardia is present. Most likely diagnosis is
Vasoconstriction in burn wound is seen in:
Blunt trauma to right side of chest, hyperresonance on right side on percussion, dyspnea, tachypnea. Heart rate-100, BP-120/80, best initial diagnostic step is
Best fluid for resuscitation of a burn patient
In a patient with multiple fractures, what is the most important initial management step?
Which of the following is the MOST SPECIFIC diagnostic marker for CSF rhinorrhea?
A 26-year-old man is brought to the emergency department with a stab wound to the right side of the back just medial to the posterior axillary line. His blood pressure is 120/80 mm Hg, pulse rate is 98 bpm, and respiration rate is 22 breaths per minute. Physical examination reveals no abdominal tenderness, guarding, or neurologic changes. Local exploration of the stab wound is performed using local anesthesia. The track to the wound ends in the paraspinal muscles. What would be the next step in management?
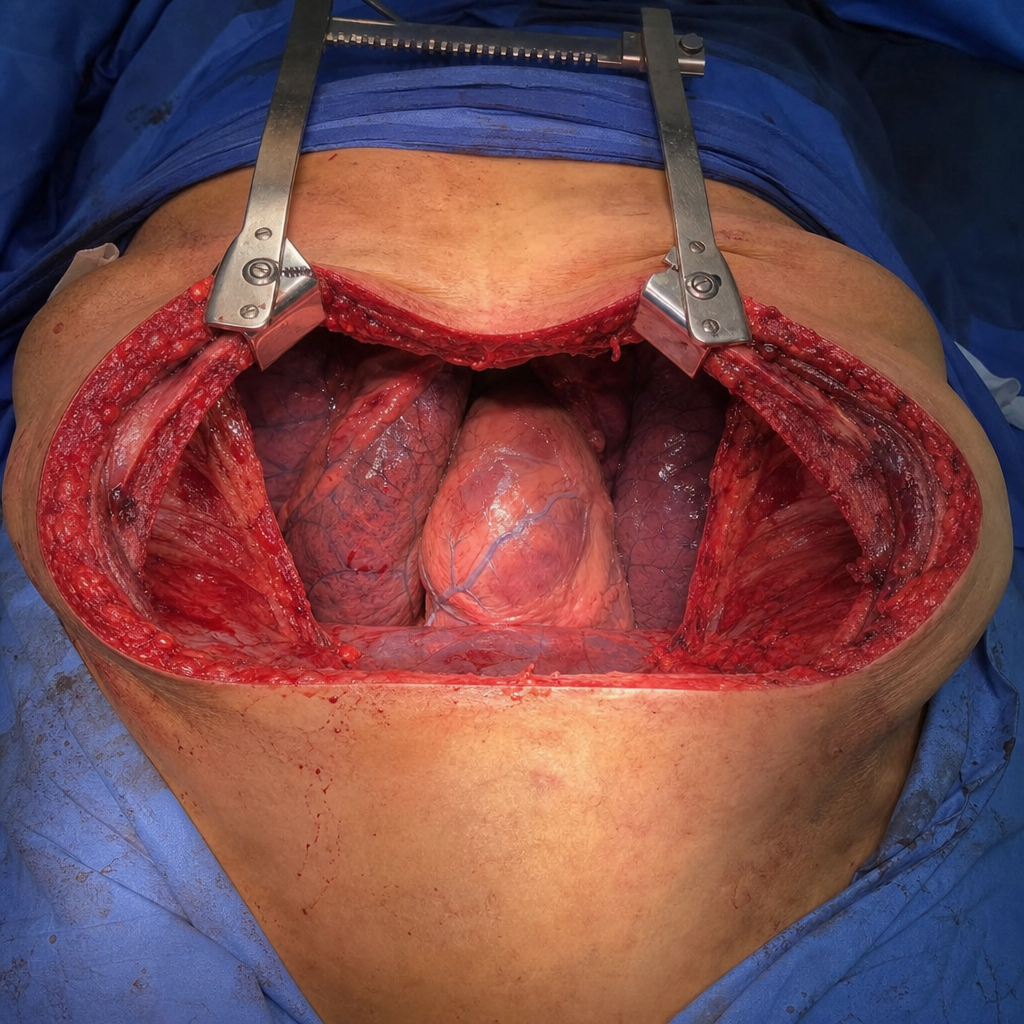
An emergency thoracotomy shown here is known as
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app