
Trauma — MCQs

On this page
Which of the following is false regarding first degree burns
Which is not an indication for thoracotomy?
Degloving injury is avulsion injury involving:
Triad following massive blood transfusion includes:
Which of the following statements about burn management is correct?
Mild head injury is having Glasgow Coma Scale of:
Rule of Nines estimates :
The best guide to adequate tissue perfusion in the fluid management of a patient with burns is to ensure a minimum hourly urine output of:
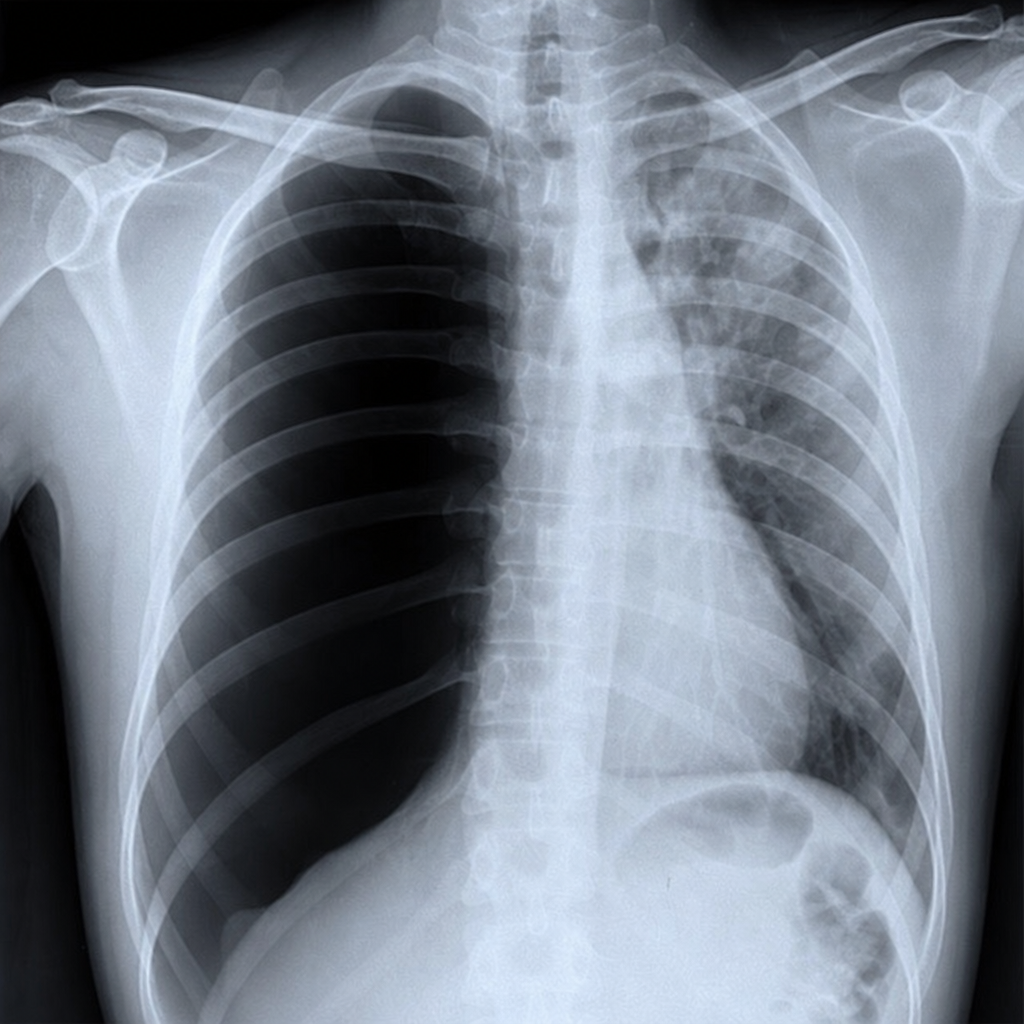
A young male met with a road traffic accident and came to the emergency department. He was evaluated and found to have BP-130/80 mm Hg, pulse rate - 88/min, RR -22/min. On auscultation, there was decreased air entry on one side with absent breath sounds. X-ray chest is given below. Your most probable diagnosis is:
A patient presents with a suspected cervical spine injury following an accident. What is the first step in management?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app