
Trauma — MCQs

On this page
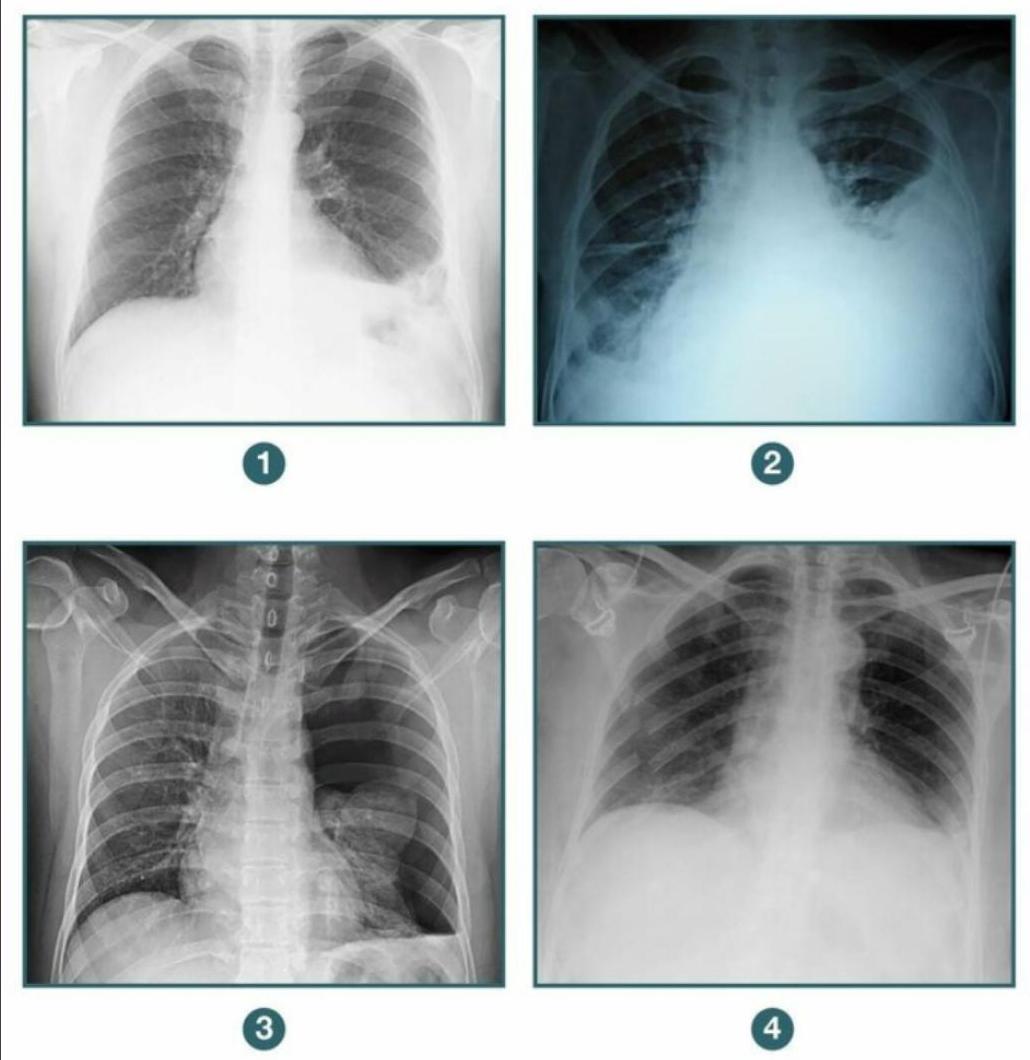
A patient presents to the casualty following blunt trauma to the chest. A chest X-ray was done showing an apparent pleural opacity. Which of the following diagnoses must be excluded before draining the opacity, because abdominal viscera may be present in the hemithorax? 1. Diaphragmatic hernia 2. Hemothorax 3. Pneumothorax 4. Flail chest
A patient presents with pneumothorax on chest x-ray. Which of the following is NOT a boundary of the triangle of safety for intercostal chest drain (ICD) insertion?
What is the correct sequence of management in a patient who presents to the casualty with an RTA? 1. Cervical spine stabilization 2. Intubation 3. IV cannulation 4. CECT
Which of these is the most life-threatening injury that can be identified by assessing the breathing component of the patient?
Incorrect statement regarding the management of frostbite:
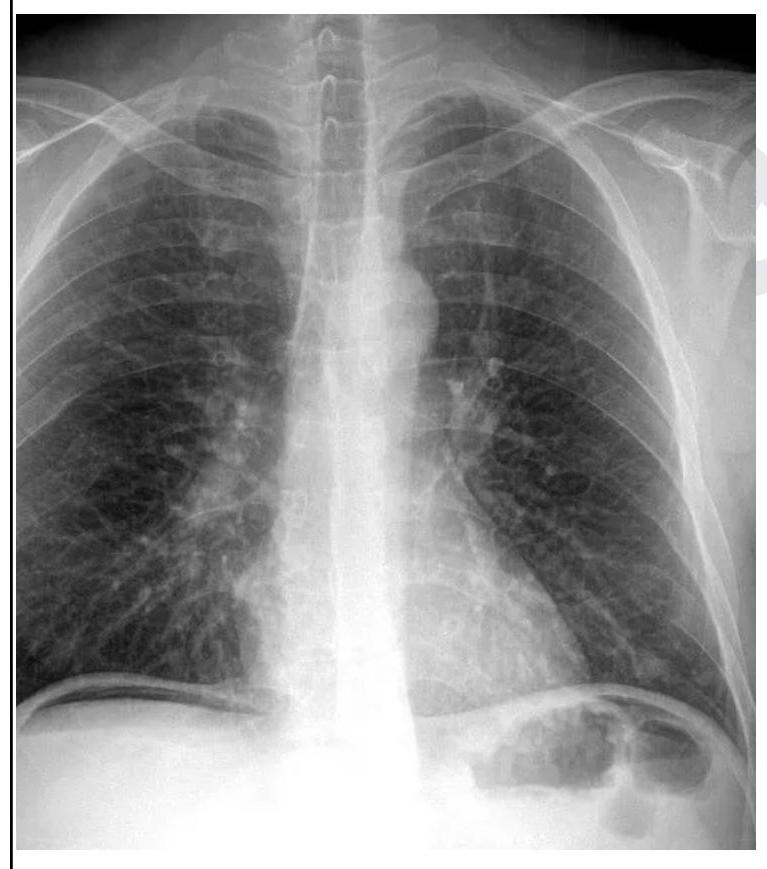
A 26 year old male patient was brought to the emergency department with abdominal pain and obstipation for 3 days. He gives a history of bull gore to the abdomen 3 days back. His chest X-ray is given below. What is the probable diagnosis?
A patient admitted after a road traffic accident is put on mechanical ventilation. He opens his eyes on verbal command and moves all four limbs spontaneously. Calculate his GCS.
A 24-year-old man is rushed to the emergency room after he was involved in a motor vehicle accident. He says that he is having difficulty breathing and has right-sided chest pain, which he describes as 8/10, sharp in character, and worse with deep inspiration. His vitals are: blood pressure 90/65 mm Hg, respiratory rate 30/min, pulse 120/min, temperature 37.2°C (99.0°F). On physical examination, patient is alert and oriented but in severe distress. There are multiple bruises over the anterior chest wall. There is also significant jugular venous distention and the presence of subcutaneous emphysema at the base of the neck. There is an absence of breath sounds on the right and hyperresonance to percussion. A bedside chest radiograph shows evidence of a collapsed right lung with a depressed right hemidiaphragm and tracheal deviation to the left. Which of the following findings is the strongest indicator of cardiogenic shock in this patient?
A 21-year-old man presents to the emergency department after sustaining a stab wound to the neck at a local farmer's market. The patient is otherwise healthy and is complaining of pain. The patient is able to offer the history himself. His temperature is 97.6°F (36.4°C), blood pressure is 120/84 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 98% on room air. Physical exam demonstrates a 3 cm laceration 1 cm inferior to the mastoid process on the right side. The patient's breath sounds are clear and he is protecting his airway. No stridor or difficulty breathing is noted. Which of the following is the most appropriate next step in the management of this patient?
A lady with 50% TBSA burn with involvement of dermis and subcutaneous tissue came to the emergency department. The burns will be classified as:
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app