
Trauma — MCQs

On this page
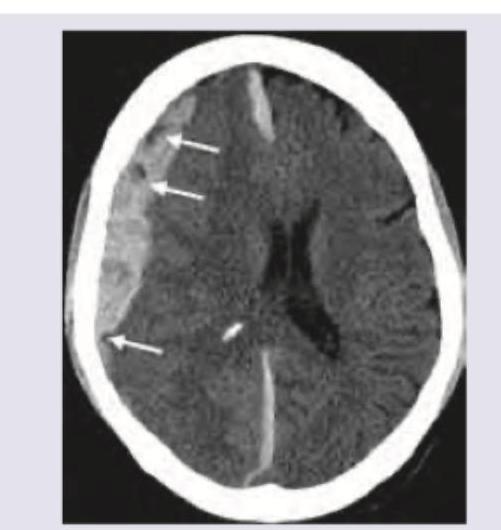
A mixed martial arts boxer lost his match by knockout. One week later, he is having daily headaches, vomiting and disorientation. On arrival in casualty $\mathrm{GCS}=7$ and fundus shows presence of papilledema. Urgent CT scan head shows?
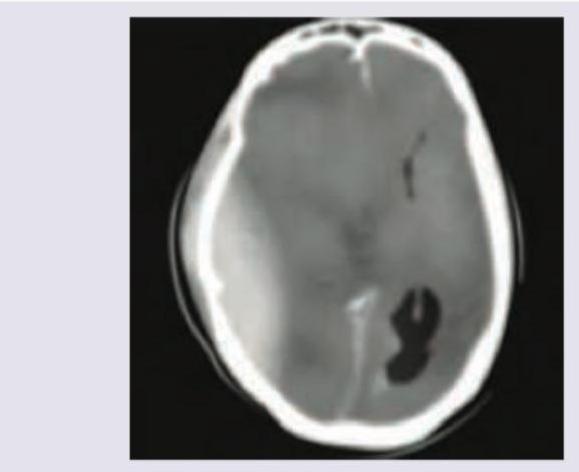
A 25-year-old patient presents in coma with GCS of 5 and extensor posturing after a bike accident. CT head was performed. Which of the following will be the best management of the patient?
A car accident patient complains of breathlessness. On examination BP is $110 / 70 \mathrm{mmHg}$ with GCS of 15/15. On examination, trachea is deviated to the right side, with reduced breath sounds in left infra-axillary area and inframammary areas. $S_{1}$ and $S_{2}$ are normal in intensity and splitting. CXR is shown below. What is the best step in management of the patient?

Which of the following statements are correct regarding ABCDE of trauma care ? I. A stands for Airway with cervical spine protection II. B stands for Breathing and ventilation III. C stands for Control of massive external haemorrhage IV. D stands for Disability (Neurological status) Select the answer using the code given below :
Which of the following statements are correct regarding primary survey/management of traumatic head injury patient? I. Ensure adequate oxygenation and circulation II. Exclude hypoglycaemia III. Check for mechanism of injury IV. Check pupil size and response Select the answer using the code given below :
A patient with head injury with a Glasgow Coma Scale of 10 is classified as :
In seat belt syndrome the most common site of bleeding is from :
A 30-year-old motorbike rider is brought to the emergency with history of a road traffic accident and altered consciousness. On secondary survey, the doctor notices presence of a bruise over the left mastoid process. The finding indicates
A 30-year-old road traffic accident victim is being taken up for emergency laparotomy for haemoperitoneum and suspected multiorgan trauma. Which one of the following will be an indication for performing damage control surgery?
Which of the following are stages of damage control surgery? 1. Patient selection 2. Control of haemorrhage 3. Resuscitation in ICU 4. Preventive surgery Select the correct answer using the code given below.
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app