
Trauma — MCQs

On this page
A head trauma patient is shown below. Diagnosis is?

All are true about the procedure shown below except: (Recent NEET Pattern 2016-17)

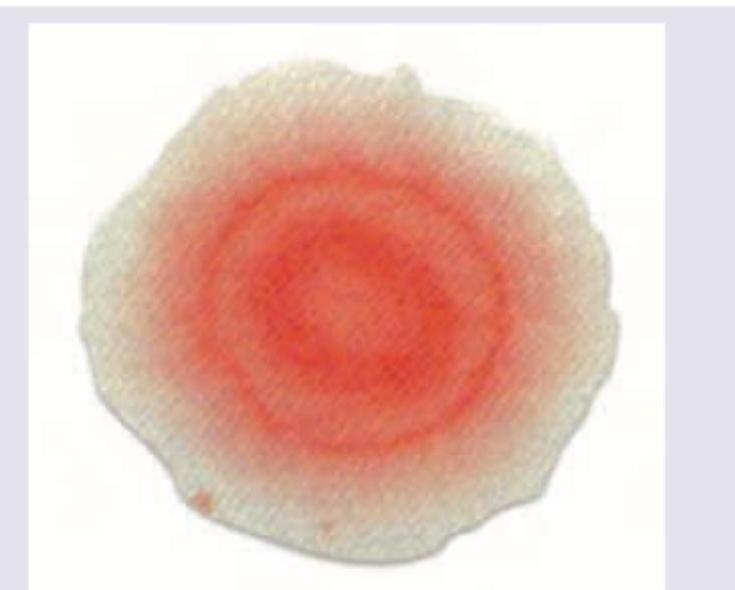
In a patient of head injury, the following sign is noted on his handkerchief. Which is the next test to confirm the diagnosis? (AIIMS Nov 2017)
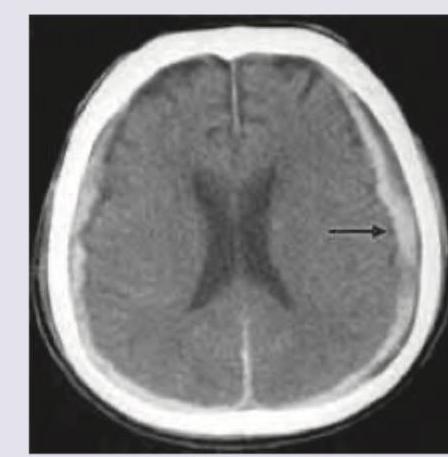
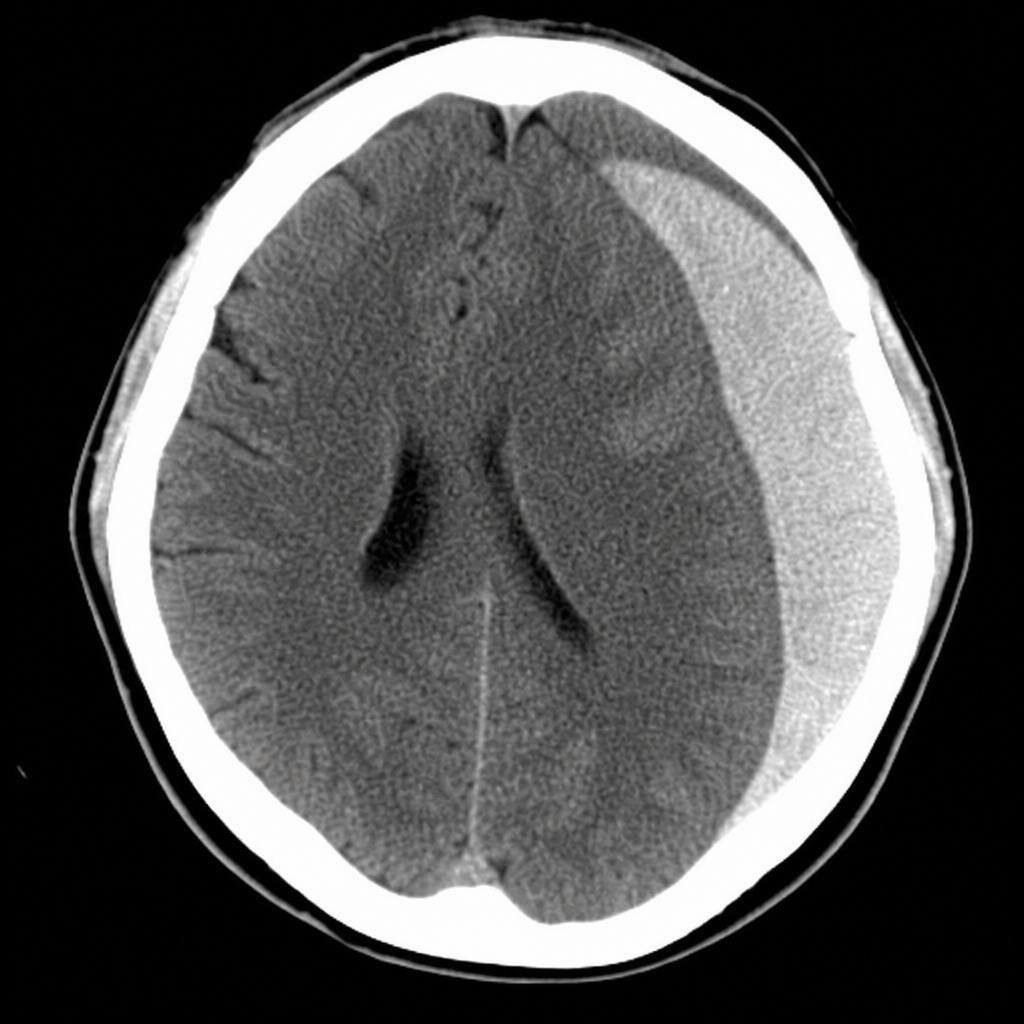
A 62-year-old diabetic female patient presented with history of progressive right sided weakness of a month duration. The patient also had speech difficulty. Fundus examination showed papilledema. 2 months ago she also had a fall in her bathroom and struck her head against the wall. The most like diagnosis based on the image given below could be?
A 25 -year-old patient presents in coma with GCS of 5 and extensor posturing after a bike accident. After airway and hemodynamic stabilization, which of the following will be the best definitive management of the patient?
A 30-year-old young male who met with a road traffic accident was brought to trauma center. On admission his BP was 90/50 mmHg, pulse rate is 150/min, SpO₂ is 80% and GCS is 8. He has multiple injuries and FAST reveals presence of blood in all quadrants. He was operated upon and his postoperative pictures are given below. Which of the following options best describe these pictures? (AIIMS Nov 2016)

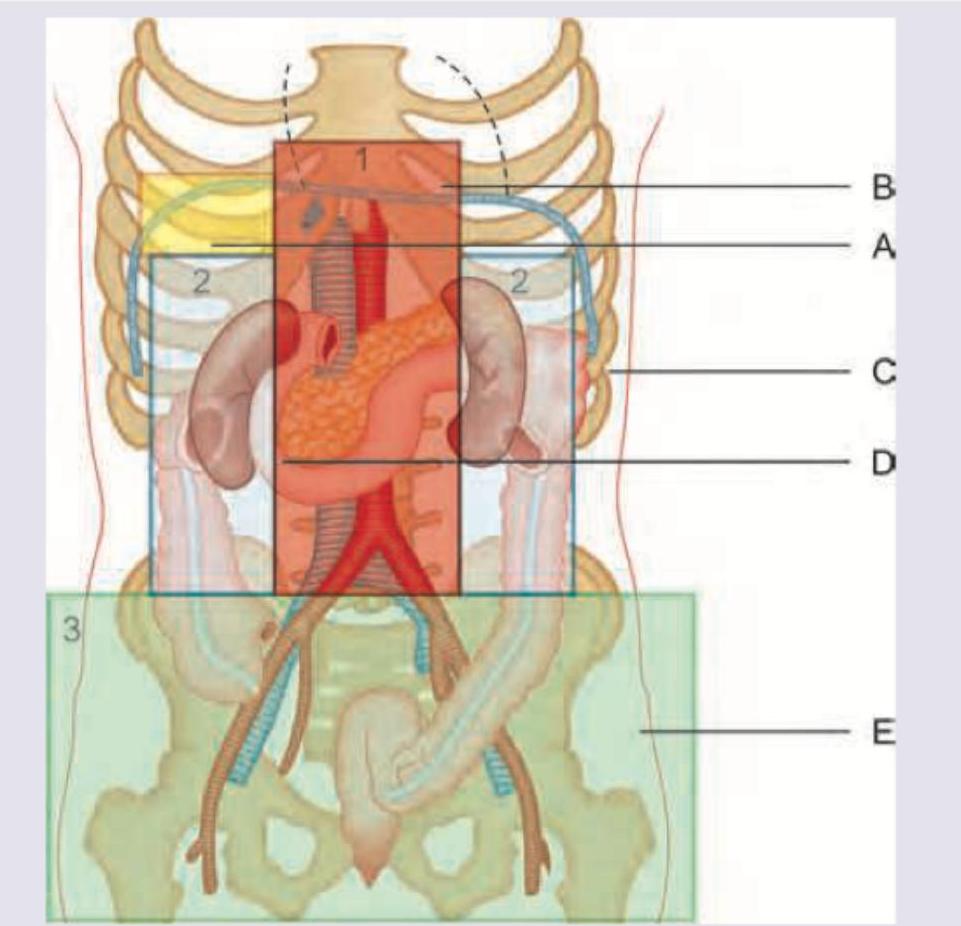
Which of the following regions marked in the picture represents zone 3 of retroperitoneal hemorrhage? (AIIMS Nov 2016)
A patient presents with severe facial burns sustained in an enclosed-space fire. On examination, there are singed nasal hairs, sooty sputum, hoarseness, and progressive facial edema. Which is the best method to secure airway and administer oxygen in case of burns shown below?

A soldier was airlifted from Siachen glacier after being trapped in an avalanche. All of the following are done in this condition except:
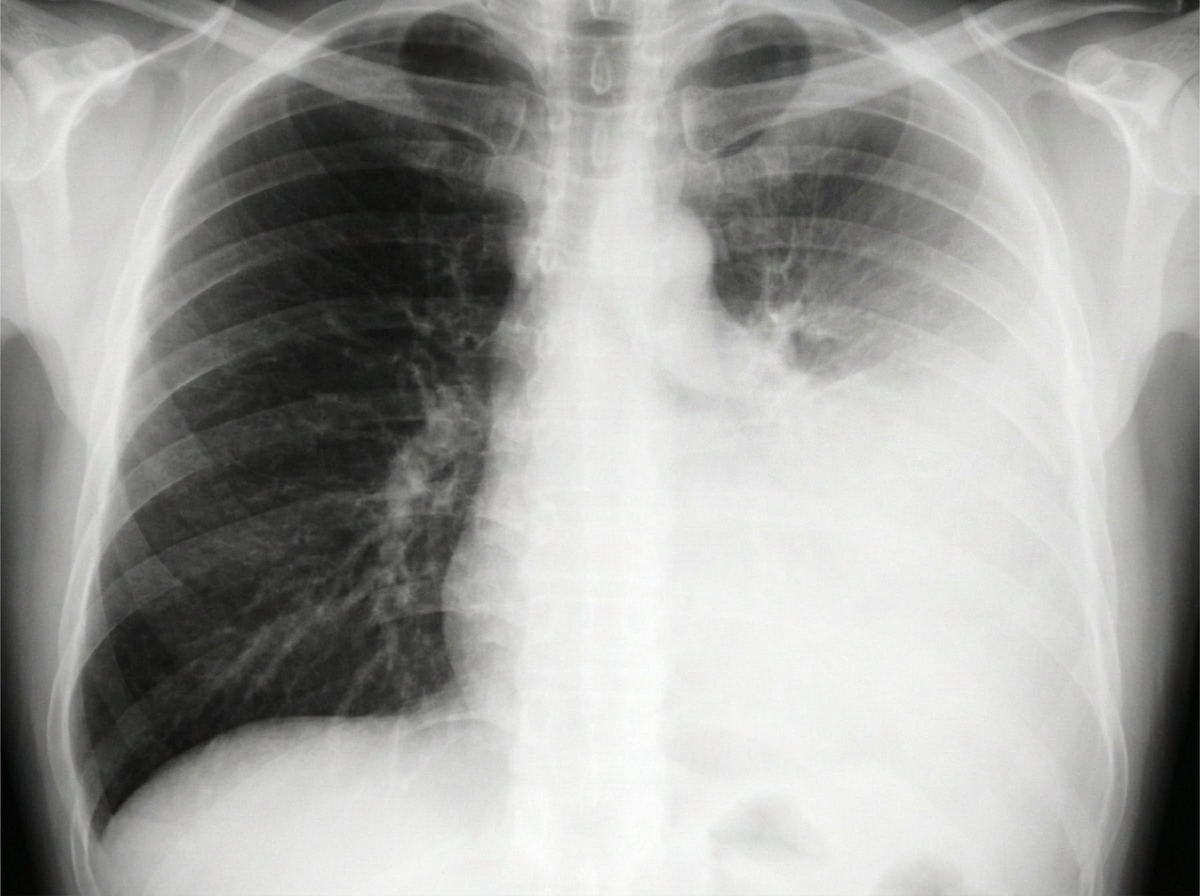
A 28-year-old male is brought to the emergency department following a road traffic accident with left-sided chest pain and breathlessness. On examination, there is decreased air entry on the left side and tracheal deviation to the right. Heart sounds are normal. The chest X-ray is shown below. What is the most appropriate immediate management?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app