
Trauma — MCQs

On this page
Which of the following is the class of shock where urine output is first decreased?
Which of the following is associated with CSF otorrhea?
A 32-year-old male presents to the emergency department 6 hours after a motor vehicle accident with hypotension (BP 80/50 mmHg), tachycardia (HR 130/min), and abdominal distension. FAST (Focused Assessment with Sonography for Trauma) shows free fluid in Morrison's pouch. What is the most appropriate immediate management?
A patient has burns involving the face, both upper limbs and front of the chest. What is the percentage of burns involved?
According to the Muir-Barclay formula, which of the following is considered the best colloid for volume replacement?
A 40-year-old male with head injury presents with respiratory distress and absent breath sounds on the right. GCS is 8/15. What is the most immediate next step in management?
After a building collapse, a patient presents with airway obstruction and mouth filled with concrete debris. BP is 90/60 mmHg, HR 105/min. A cricothyrotomy is performed. Which of the following statements regarding this procedure is true?
A 30-year-old female was brought to the emergency room after a fire. On examination, full-thickness burns and deep partial-thickness burns were present involving the lower limb circumferentially. A procedure was performed to relieve vascular compromise. Identify the procedure?
A 40-year-old male presents to the emergency department with severe respiratory distress, BP: 70/59 mmHg, tracheal deviation to the right, distended neck veins, and absent breath sounds on the left side. These findings are suggestive of a tension pneumothorax. What is the most appropriate immediate next step in management?
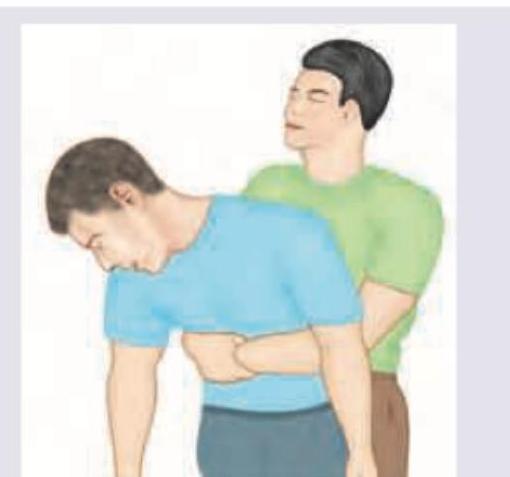
Which of the following correctly describes the hand placement and direction of force for the technique visibly depicted in the image?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app