
Trauma — MCQs

On this page
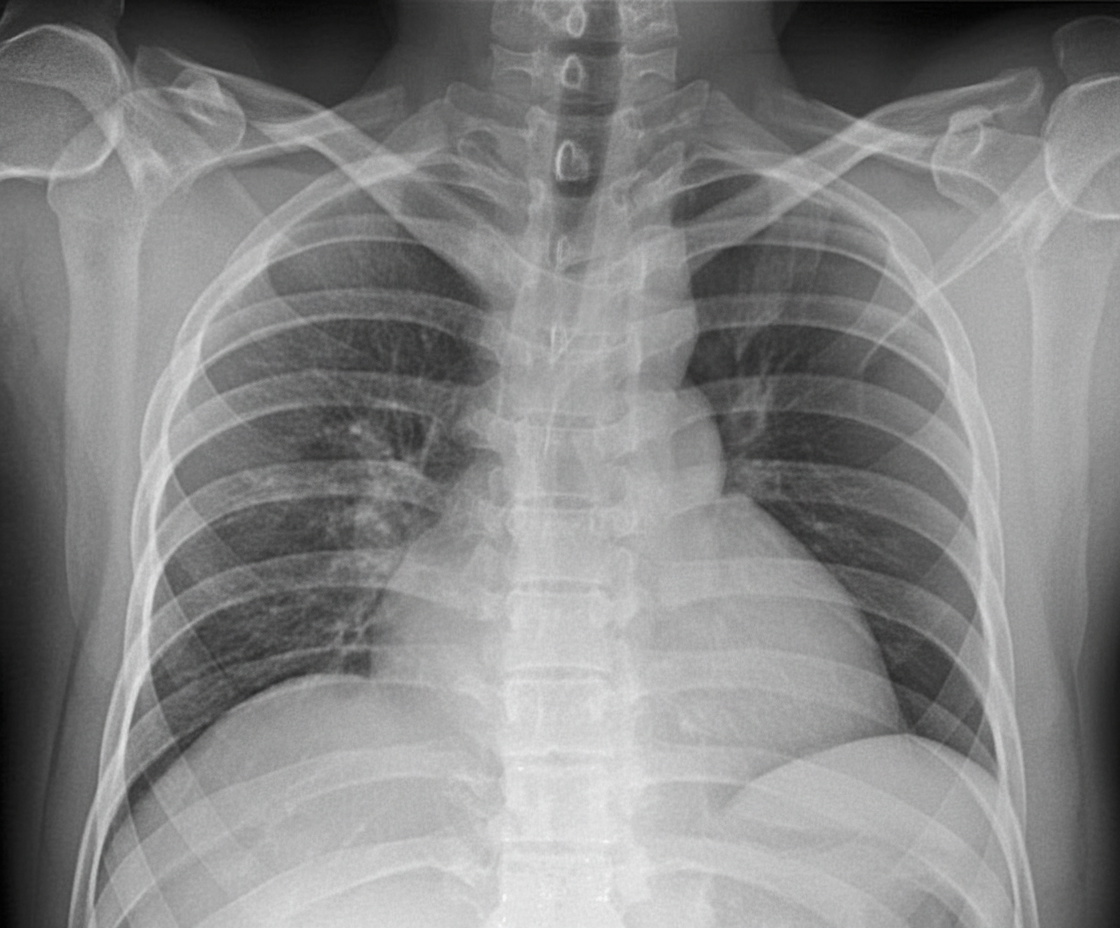
Under which category would you classify this injury?

After trauma, hypovolemic shock can be due to all EXCEPT:
A patient involved in a road traffic accident presents with a pulse rate of 96 beats per minute, a systolic blood pressure of 68 mmHg, and a respiratory rate of 20 breaths per minute. The patient is confused. What is the likely percentage of blood loss?
Floating maxilla is typically found in which type of fracture?
A male patient with blunt abdominal trauma is hemodynamically stable. What is the next line of management?
A 23-year-old man was involved in a motor vehicle accident and presents with decreased breath sounds on the left side, tracheal deviation to the right, and hypotension. What is the diagnosis?
Which of the following statements concerning topical antimicrobials in common use today is/are true?
An 18-year-old man presents after a motorcycle accident with a history of brief unresponsiveness. Skull films show a left temporal bone fracture. After the x-ray, he loses consciousness and develops left pupil dilation. What is the most likely diagnosis?
Which statement is true about aortic transaction?
A 5-year-old child has burns on the body surface equivalent to the size of their palm. What is the estimated percentage of total body surface area affected by the burns?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app