
Trauma — MCQs

On this page
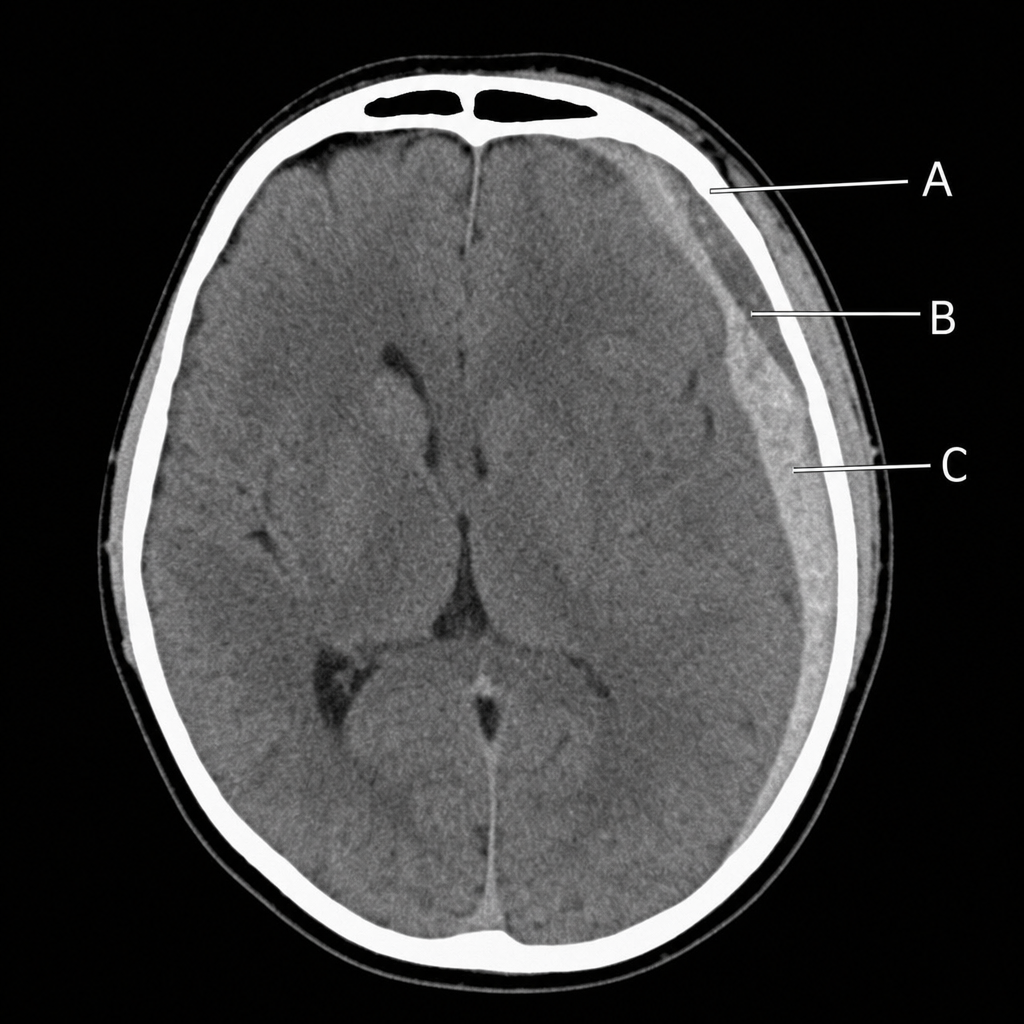
A young boy sustains a head injury from being hit by a ball on the left side of his head, leading to a period of unconsciousness. He regains consciousness but becomes confused shortly after. Upon examination at the hospital, his left pupil is found to be dilated. NCCT head reveals specific findings. Which of the following marked structures on the NCCT head is most likely responsible for the observed left pupil dilation?
Isolated splenic or hepatic injury in a child is most commonly managed by?
What percentage of severe trauma is associated with extradural hematoma?
A patient with a head injury presents with a Glasgow Coma Scale of 8, a mid-face fracture, cyanosis, decreased breathing with frequent apnea, and hypoxia. What is the most appropriate method for airway maintenance?
A patient is in shock with a gross comminuted fracture. What is the immediate treatment?
Injury to the aorta causing aortic rupture is most commonly seen in which of the following scenarios?
A 42-year-old man involved in a house fire presents with singed nose hairs and facial burns. Direct laryngoscopy reveals pharyngeal edema and mucosal sloughing. He has 60% total body surface area burns. What is the next most appropriate step in managing this patient?
Characteristic features of superficial burns are all, except:
A patient with a history of fall presents weeks later with headache and progressive neurological deterioration. What is the diagnosis?
Heimlich valve is used for the drainage of which of the following conditions?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app