
Trauma — MCQs

On this page
Which of the following statements is false regarding a epidural hematoma?
What is an absolute contraindication for tooth extraction when related to a fracture line?
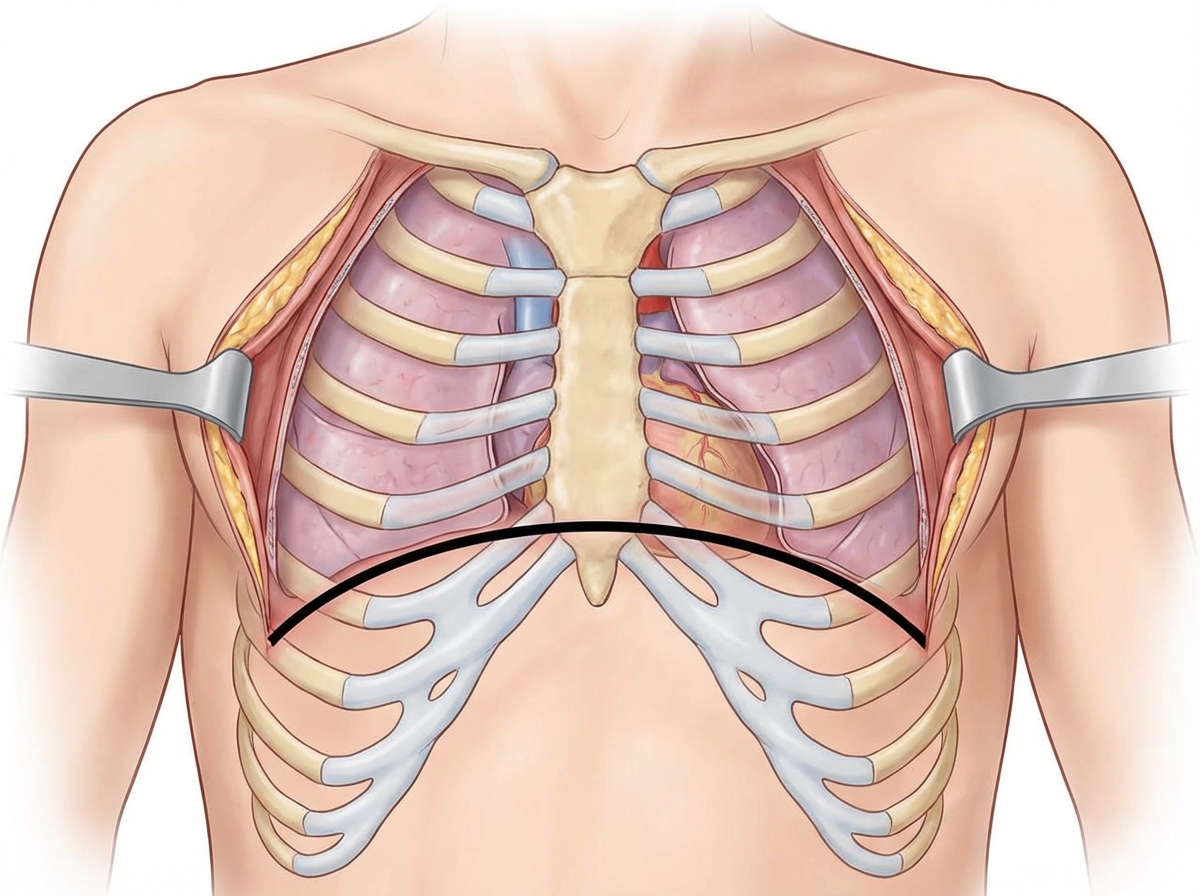
What is the name of the emergency thoracotomy procedure illustrated?
A 70 kg female has 50% burns and an inhalation burn injury. What is the fluid requirement in the first 8 hours according to the Parkland formula?
A male patient is admitted following a fall from height. On arrival his Glasgow Coma Scale score is 5/15 and he is therefore intubated. During primary resuscitation, a chest film is taken which shows a widened mediastinum and right-sided deviation of the trachea. What is the most likely diagnosis?
A man presented with fractures of 4th to 10th ribs and respiratory distress after a Road Traffic Accident. He is diagnosed to have flail chest. What is the recommended management?
A patient admitted to the casualty department after a road traffic accident shows bruising behind the mastoid. This sign is known as?
What is the most important aspect of management of burn injury in the first 24 hours?
A 40-year-old man presents to the emergency department one hour after a motor vehicle accident with severe maxillofacial trauma. His pulse rate is 120/min, BP is 100/70 mm Hg, and SpO2 is 80% on oxygen. What is the immediate management?
In a trauma patient experiencing shock, an initial 500ml infusion of normal saline over 5-10 minutes resulted in a temporary blood pressure improvement that lasted only 15 minutes before it began to fall again. What is your inference?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app