
Trauma — MCQs

On this page
Subdural hematoma most commonly results from?
When is emergency endotracheal intubation indicated?
Fracture at the angle of the mandible most commonly involves which tooth?
Which of the following does NOT require hospitalization?
A 35-year-old chemical factory worker presents to the emergency department after a sudden splash of an unknown chemical onto his hands and feet. Which of the following statements is true regarding the management of chemical burns, except?
What is the initial management for a patient with 40% blood volume loss?
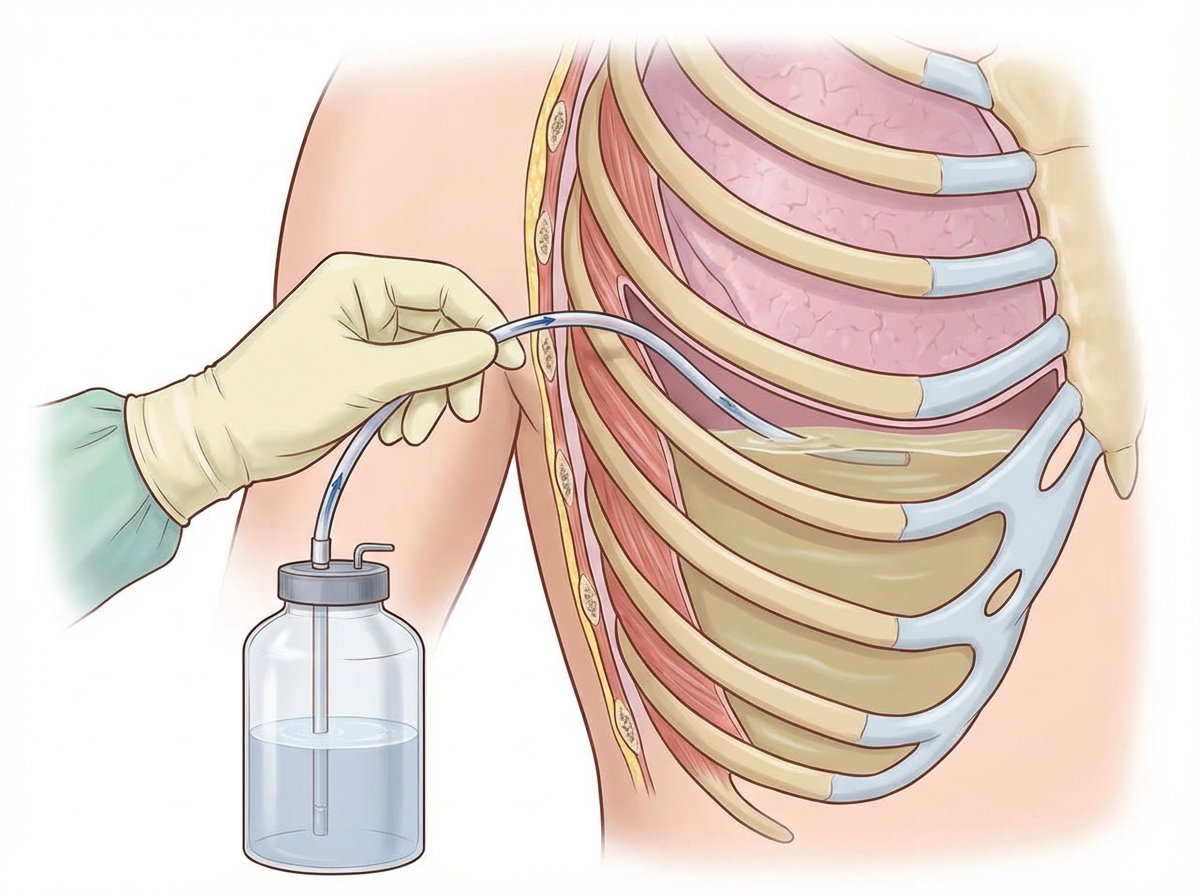
The above procedure is indicated in all of the following conditions EXCEPT?
Massive blood transfusion is defined as:
If a fracture of the mandible occurs distal to a lost tooth, what is the treatment of choice?
A young male presented with dyspnea, bleeding, and petechial hemorrhage in the chest 2 days following a fracture of the shaft of the right femur. What is the most likely cause?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app