
Trauma — MCQs

On this page
All of the following are true about the CRASH-2 trial except:
In third-degree burns, which of the following findings is typically absent?
A 3-year-old child suffers from a burn injury involving the face, including the scalp, both buttocks, and circumferentially around both thighs. What is the Total Body Surface Area (TBSA) involved?
In a condylar fracture with greater than 5 mm of overlapping and greater than 37 degrees of angulation of the fracture segment, what is the line of treatment?
Which of the following is NOT true regarding burn patients?
What is the degree of this burn shown below?

Which among the following topical agents used in burns can cause acidosis?
Which of the following is NOT a criterion for admission to a burn ward?
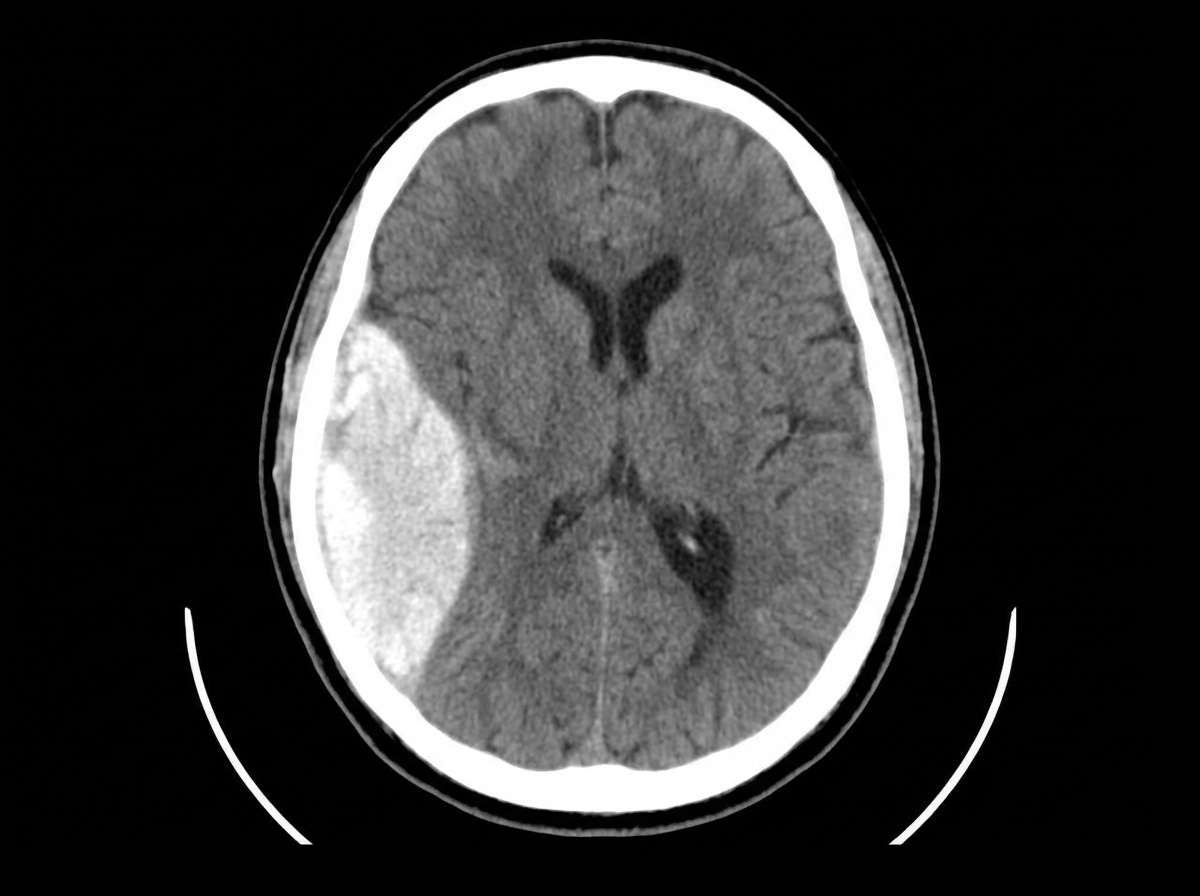
A 30-year-old patient with a head injury presented to the emergency department. NCCT findings are provided. All of the following are true about this condition except:
After an open injury, what is the optimum time for nerve suture?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app