
Trauma — MCQs

On this page
What is the treatment for cardiac tamponade?
Which of the following statements is true about the management of burns?
In lingual splaying of guardsman fracture with ORIF, which is the clinical feature?
What is the investigation of choice in pancreatic trauma?
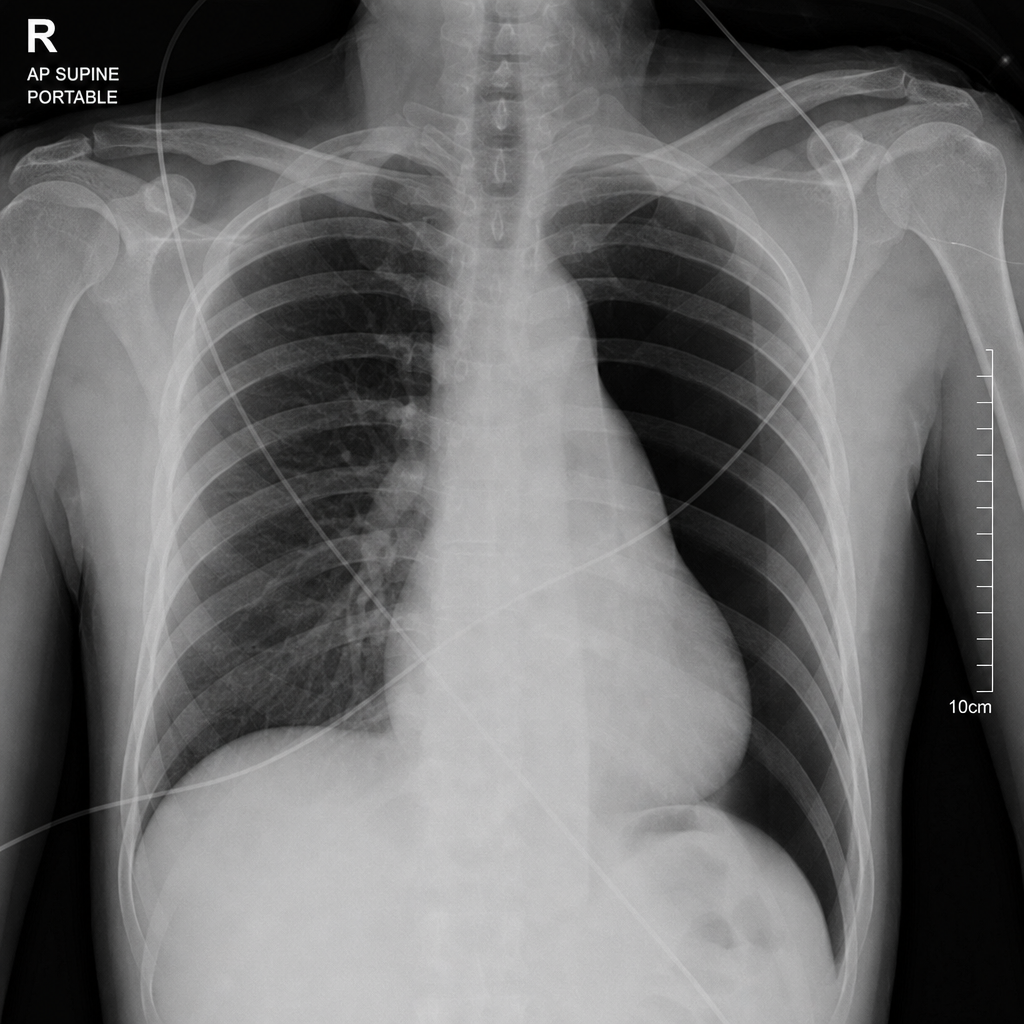
A patient is brought to the emergency department after an assault, presenting with unconsciousness, HR 104/min, BP 90/64mmHg, and RR 26/min. Examination reveals a penetrating wound approximately 4-5 cm from the midline in the right 5th intercostal space. Following stabilization, a chest tube is inserted but a persistent air leak and failure of lung re-expansion are noted. Subsequent X-ray is obtained. What is the most likely interpretation?
Triple H therapy in the management of subarachnoid hemorrhage includes all except?
A 25-year-old woman presents to the emergency department with multiple gunshot wounds to the abdomen. Her blood pressure is 70 mm Hg and her abdomen is massively distended. Large intravenous lines are placed, and a nasogastric tube and Foley catheter are inserted. The patient is taken immediately to the operating room. After 2 L of normal saline infusion, her blood pressure remains 75/0 mm Hg, pulse rate is 140 bpm, and respiration rate is 30 breaths per minute. What is the next step in management?
Burns with destruction of the epidermis and papillary dermis are classified as which degree?
A 40-year-old female patient complains of excessive bleeding following a road traffic accident 6 hours ago. She presents with altered mental status, a blood lactate level of 2.5 mmol/L, reduced urine output, blood pressure of 80/50 mmHg, pulse of 130 bpm, and a respiratory rate of 24/minute. In which stage of shock is this patient?
In limb reconstruction, what is the first step undertaken?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app