
Trauma — MCQs

On this page
A 28-year-old male involved in a motorcycle accident presents with severe respiratory distress, hypotension (BP 80/40 mm Hg), cyanosis, epistaxis, an open femur fracture, and decreased breath sounds on the right side. What is the initial management priority?
Early reversible shock is characterized by?
What is the degree of burns in a patient presenting with blister formation?
Hutchinson's pupil is characterised by:
Crush syndrome is managed by which of the following measures?
Base of skull fracture involves the petrous temporal bone. Which of the following is an important sign?
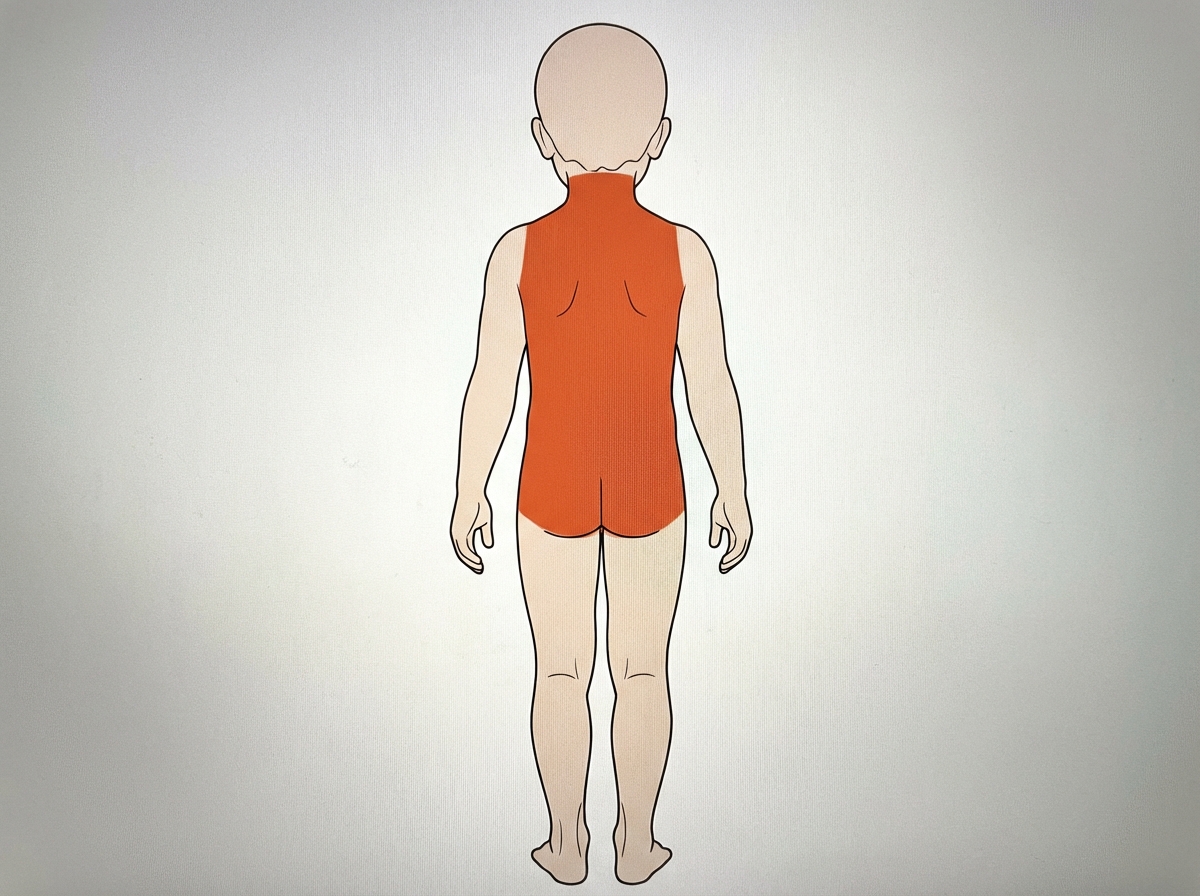
A 10-year-old boy sustained a burn injury on his back. What percentage of his Total Body Surface Area (TBSA) does this injury represent?
A 40-year-old man with severe maxillofacial trauma following a motor vehicle accident presents to the emergency department one hour after the incident. His vital signs are: Pulse rate 120/min, BP 100/70 mm Hg, and SpO2 80% on oxygen. What is the most appropriate immediate management?
A patient with head injury opens eyes on painful stimulus, uses inappropriate words and localizes pain. What is his GCS score?
A 42-year-old man presents with fractures of the left tenth, eleventh, and twelfth ribs and left tibia and fibula fractures following trauma. His vital signs are: blood pressure 120/90 mm Hg, pulse rate 100 bpm, and respiration rate 24 breaths per minute. He has hematuria and left flank pain. Intravenous pyelography shows no excretion from the left kidney but normal excretion from the right. What is the next step in management?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app