
Trauma — MCQs

On this page
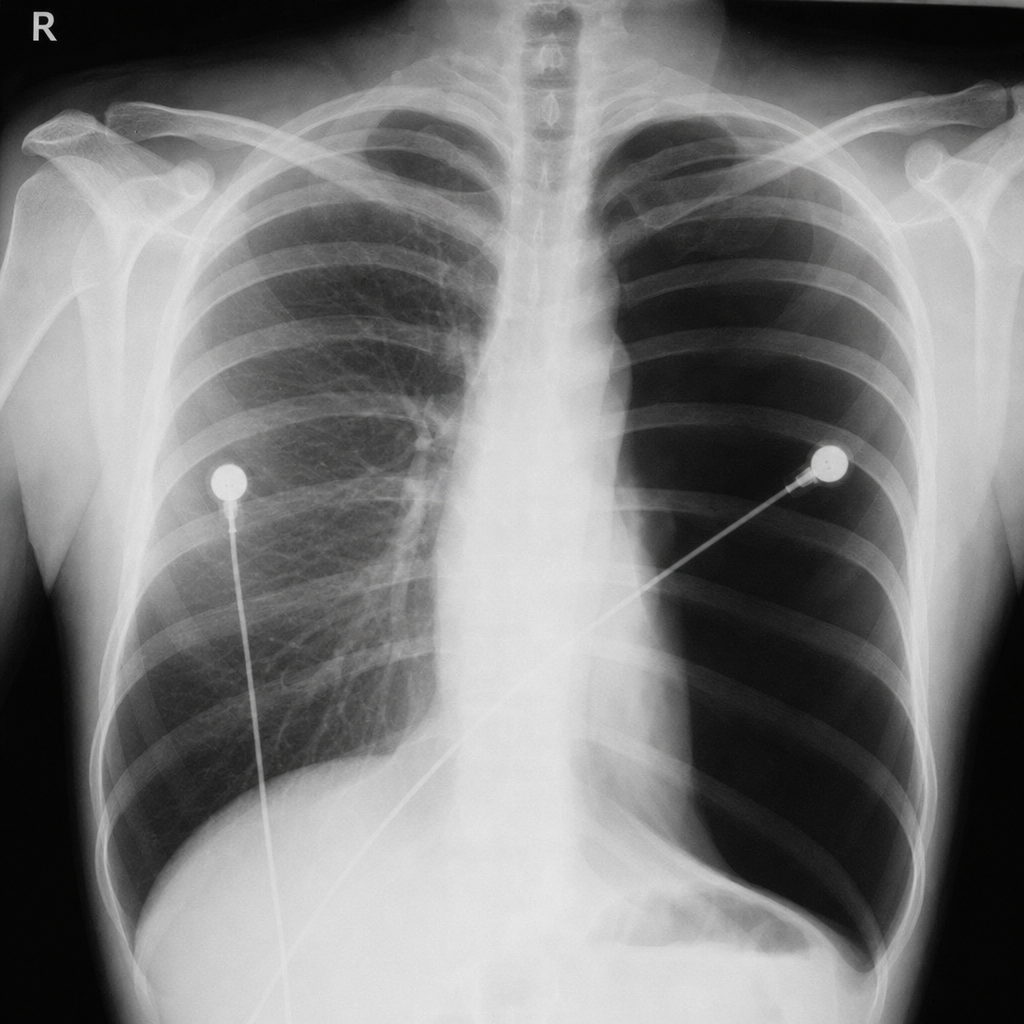
A 20-year-old male patient presents to the ER with severe dyspnea. On examination, there is severe tachycardia, hypotension, and distended neck veins. A chest x-ray is provided. What is the most likely diagnosis?
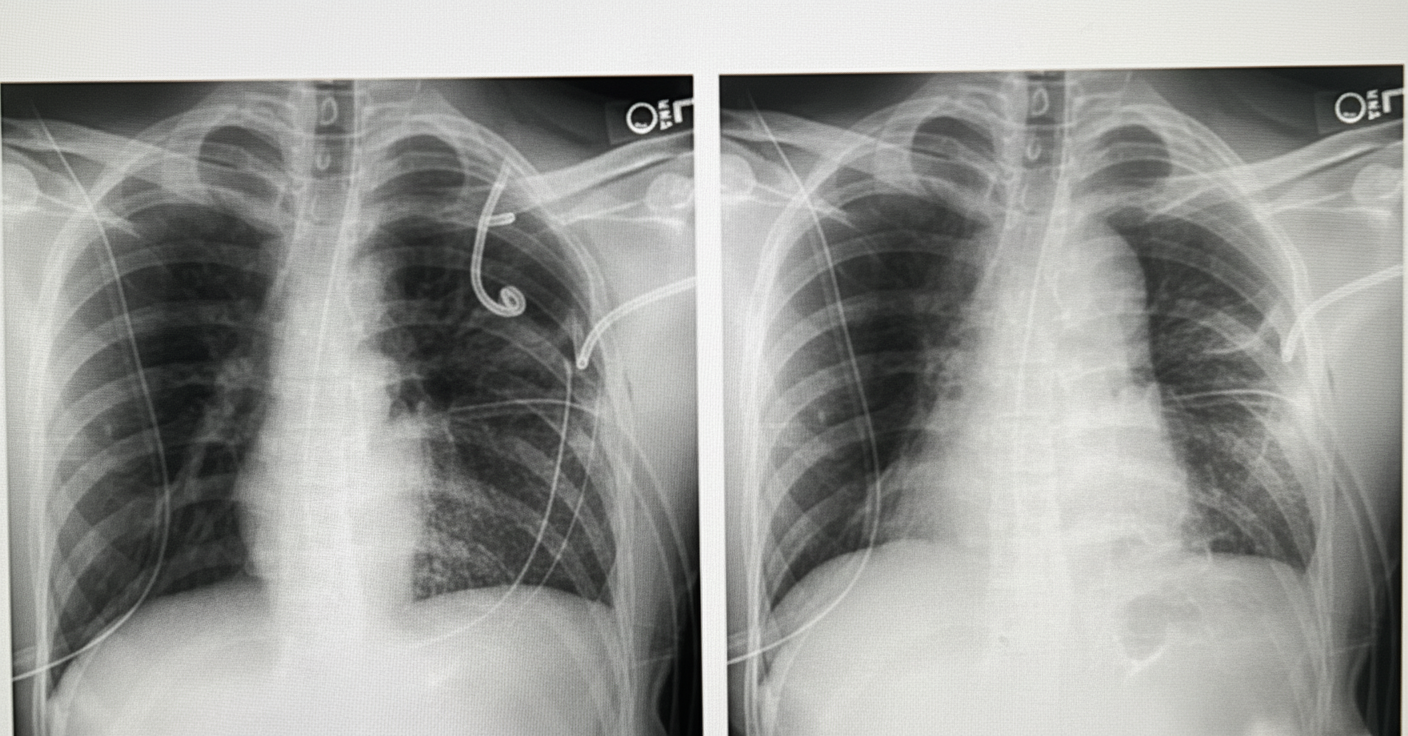
A 50-year-old patient presents to the ER with a history of a road traffic accident. The patient is unconscious. e-FAST revealed fluid in the pelvis. Chest X-ray is provided. What is the most likely diagnosis?
In an injured patient with hypovolemia, which parameter primarily guides intravenous fluid administration?
Exposure treatment is done for burns of which body part?
Which anatomical site is typically affected by a Curling's ulcer?
A patient sustained traumatic injury to major abdominal vessels. It has been planned to explore the suprarenal aorta, the celiac axis, the superior mesenteric artery, and the left renal artery. Which maneuver is recommended for exposure of all these structures?
All of the following are true about diffuse axonal injuries except?
A 30-year-old male presents after an accident with inability to move his legs and pass urine. Trauma to the cervical spine is suspected. What is the best initial approach?
What is true about Flail chest?
What is the Muirs and Barclays formula used for?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app