
Trauma — MCQs

On this page
A dermoepidermal burn is classified as which degree of burn?
A 33-year-old person involved in a motor vehicle accident develops an extradural hematoma. What is the most likely vessel to be bleeding?
A 15-year-old boy sustains 20% total body surface area (TBSA) burns. After primary assessment, burn dressing with silver nitrate is applied on his wounds. Which of the following is associated with the use of silver nitrate?
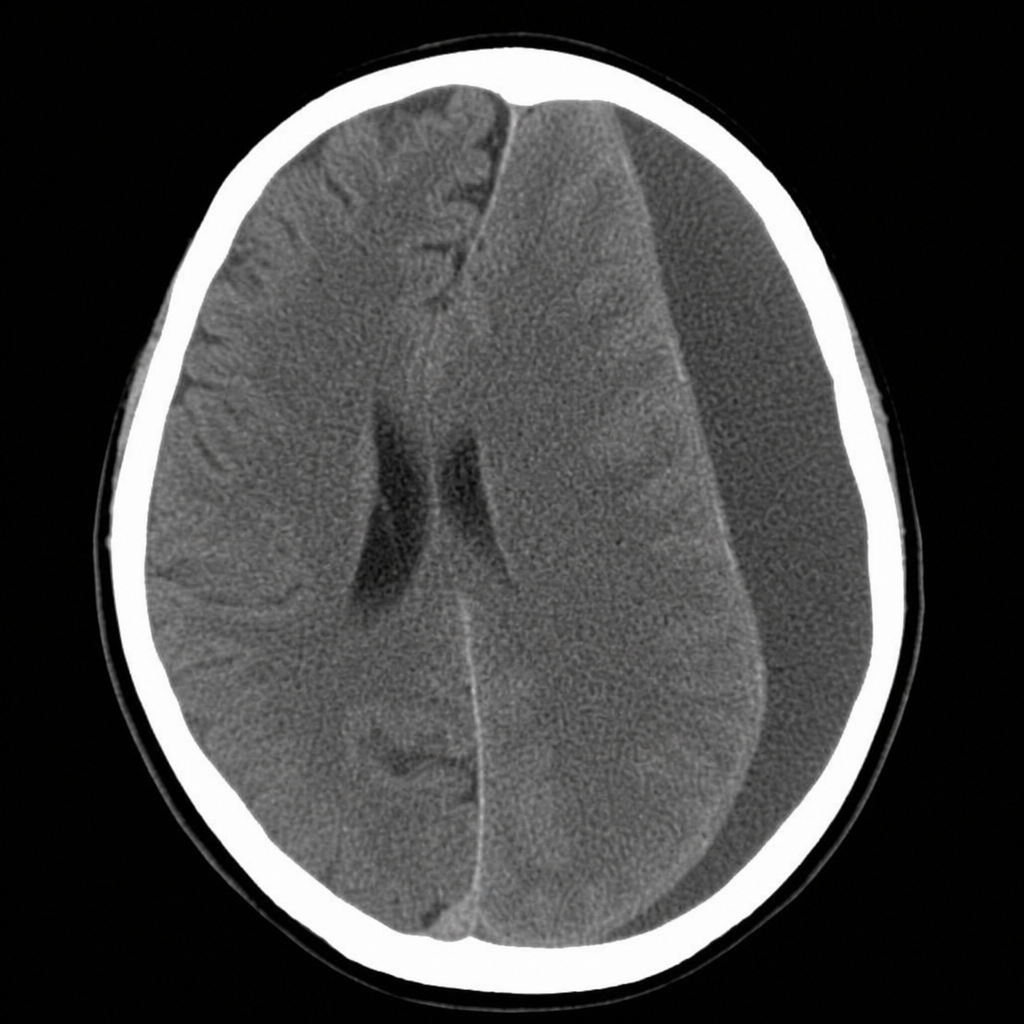
A 60-year-old patient was brought to the emergency. NCCT head was performed and findings are given below. All of the following are true about this condition except:
Class III hemorrhage is defined as blood loss up to?
Which of the following is not a component of the crush syndrome?
Decision regarding surgery in a case of hemothorax due to blunt trauma chest should be based on which of the following?
Hypertonic saline is not indicated in which of the following conditions?
Diplopia is most common with which of the following injuries?
A 40-year-old woman was involved in a car crash and was unconscious for 5 minutes. X-ray revealed a depressed fracture in the frontal region. Which of the following statements is true of skull fracture?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app