
Trauma — MCQs

On this page
What is a suprazygomatic fracture?
Which of the following structures remains intact in a closed head injury?
Which of the following statements about shock is true?
A 25-year-old male presents to the Emergency Department with a history of a road traffic accident two hours prior. The patient is hemodynamically stable. The abdomen is soft. On catheterization of the bladder, hematuria is noticed. What is the next step in management?
Which type of shock is typically seen in patients with severe burns?
From the following list, choose the appropriate order of priorities in the management of a patient with polytrauma: 1. Control of external haemorrhage 2. Intravenous infusion and transfusion 3. Maintenance of patent airway 4. Relief of a tension pneumothorax 5. Splinting of fractures.
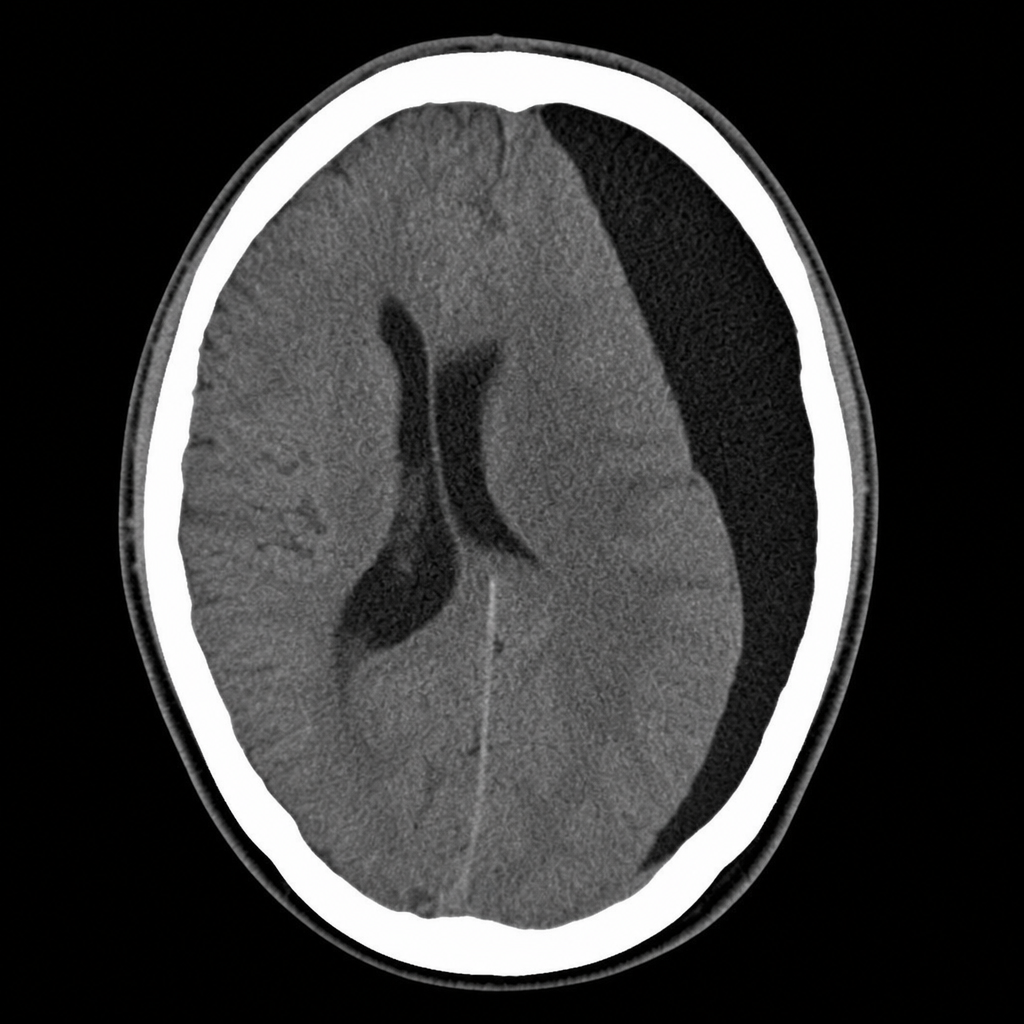
A 65-year-old male presents with mental confusion and poor physical coordination three weeks after a minor head injury. Radiographic examination reveals bleeding over the right cerebral hemisphere. What is the most likely diagnosis?
Which is the next best management for a patient with the following CT scan report?
What is the treatment of choice for a gunshot injury?
What is the safest strategy for treating a patient with an inhalational burn injury who presents within 4-5 hours?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app