
Trauma — MCQs

On this page
Which of the following is most commonly associated with full-thickness burns?
A 5-year-old child falls and sustains a laceration to the forehead. Which of the following statements is true about lacerations?
A 45-year-old male presents with severe abdominal pain following a high-speed car accident. On examination, there is tenderness in the right upper quadrant and epigastrium with guarding. What is the most likely organ to be injured?
What is the typical color change observed in contusions as they progress over time?
What is the best initial management for a burn patient with a suspected inhalation injury?
A patient presents to the emergency department following blunt abdominal trauma with severe abdominal pain, a pulse of 112 beats per minute, and a systolic blood pressure of 80 mmHg. Based on ATLS principles, what is the immediate next step in management?
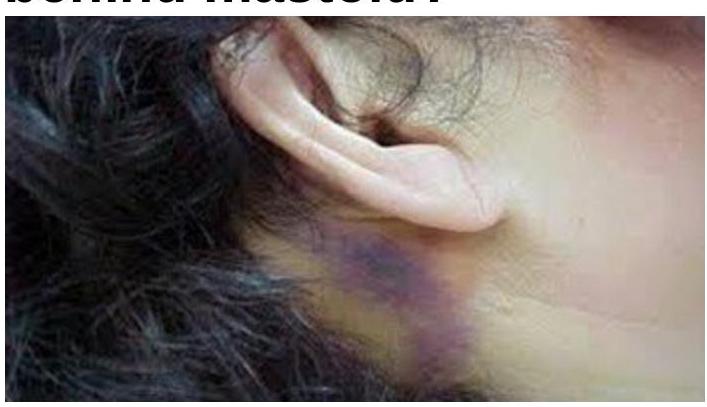
What does a bluish-purple discoloration behind the mastoid indicate?
What is the most common indication for performing a tracheostomy?
Estimate volume of Ringer lactate in first 8 hours for a 50 kg male with 40% TBSA second-degree burns?
What is the absolute pressure threshold for surgical intervention in compartment syndrome?
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app