
Transplant Surgery — MCQs

On this page
What is the most common malignancy observed in renal transplant recipients?
What is the most common infection within one month post-renal transplant?
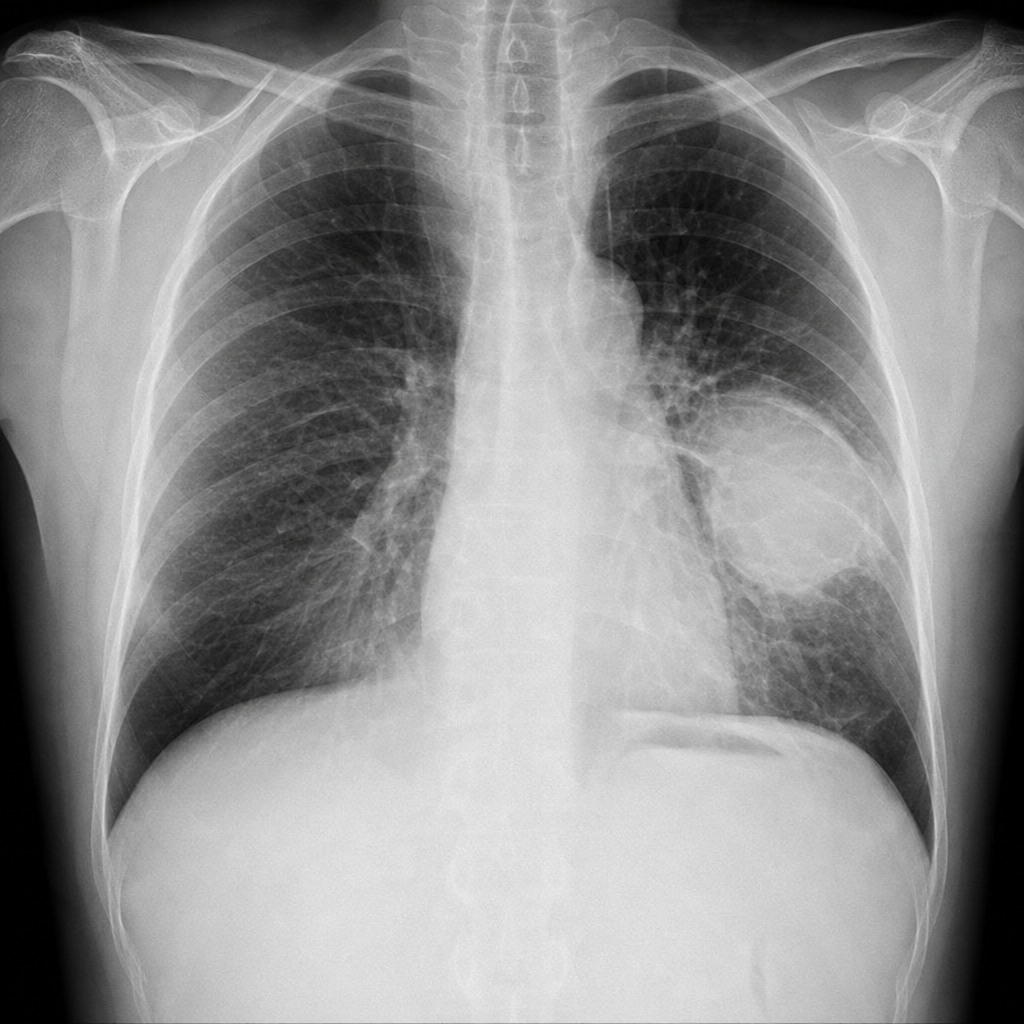
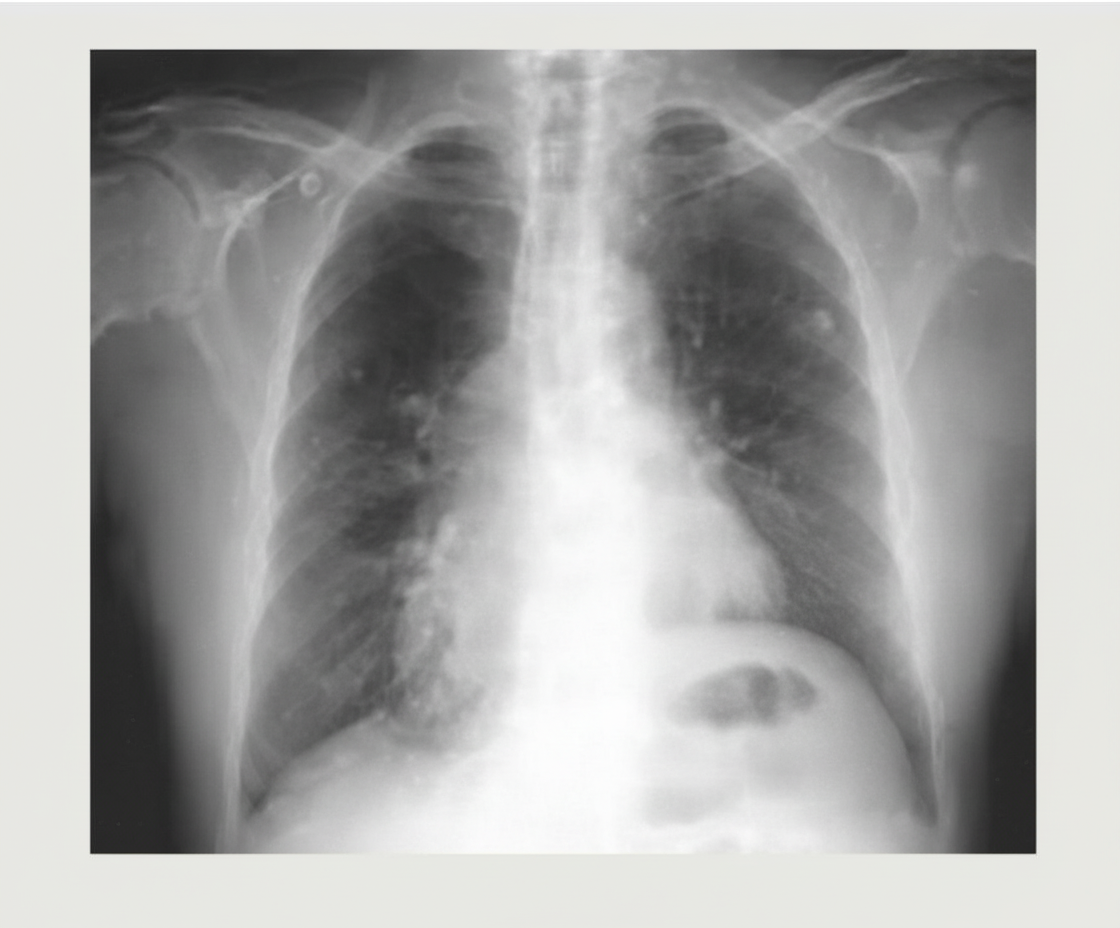
A 32-year-old male who underwent a lung transplant 1 year ago, with a history of acute rejection requiring increased immunosuppression, now presents with low-grade fever, generalized fatigue, and weight loss. Chest x-rays are obtained. What is the most likely diagnosis?
Which type of Maastricht classification is a brought dead patient?
A 32-year-old male who underwent a lung transplant 1 year ago, with a history of acute rejection requiring increased immunosuppression, now presents with low-grade fever, generalized fatigue, and weight loss. Chest x-rays are obtained. What is the most likely diagnosis?
What is the commonest cause of mortality in liver transplant operations?
Hypothermia (0deg to 4deg C) is a critical component of successful organ cold storage because:
Transplantation of which one of the following organs is most often associated with hyper-acute rejection?
What is considered a contraindication for liver transplant?
What is the site of transplantation in islet cell transplantation for diabetes mellitus?
Practice by Chapter
Immunology of Transplantation
Practice Questions
Immunosuppression
Practice Questions
Organ Procurement
Practice Questions
Kidney Transplantation
Practice Questions
Liver Transplantation
Practice Questions
Pancreas Transplantation
Practice Questions
Heart Transplantation
Practice Questions
Lung Transplantation
Practice Questions
Small Bowel Transplantation
Practice Questions
Complications of Transplantation
Practice Questions
Transplantation in Special Populations
Practice Questions
Ethical Issues in Transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app