
Surgical Infections — MCQs

On this page
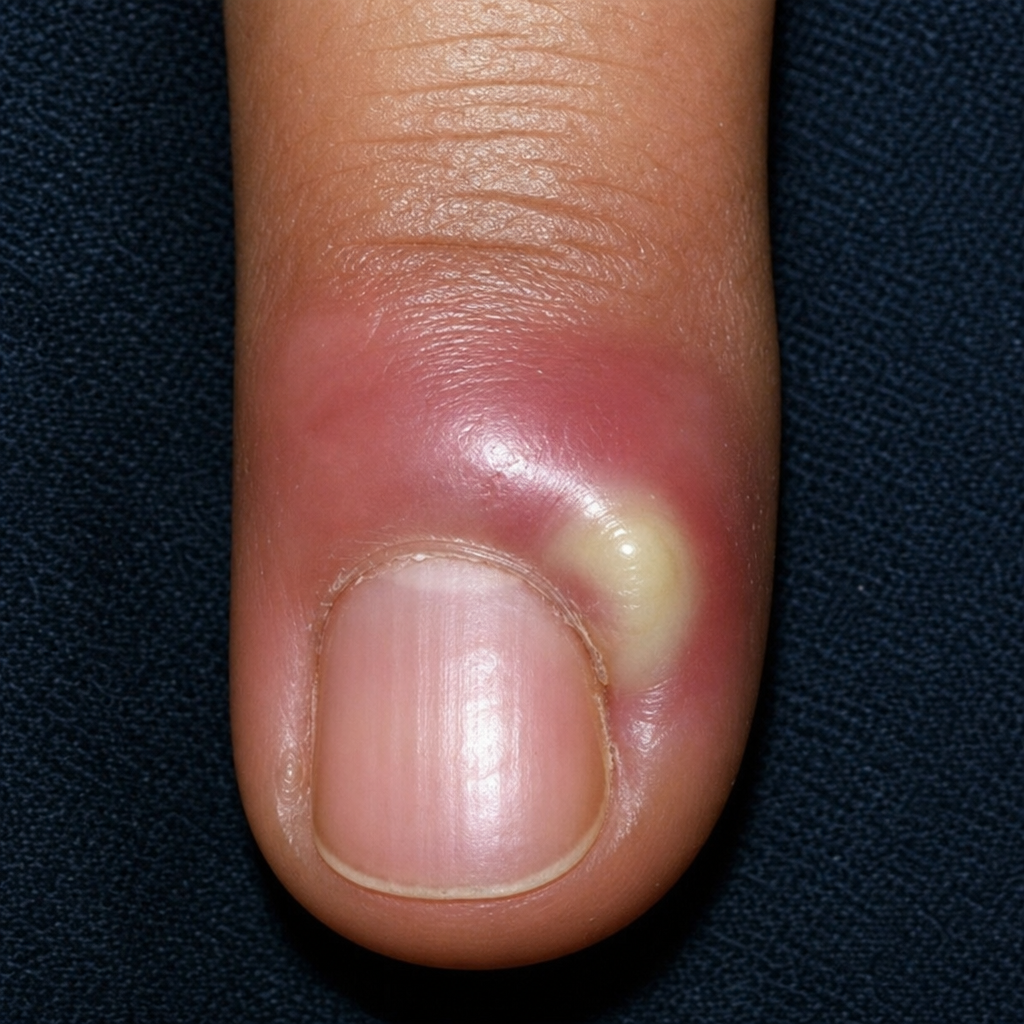
All are true about the image shown except:
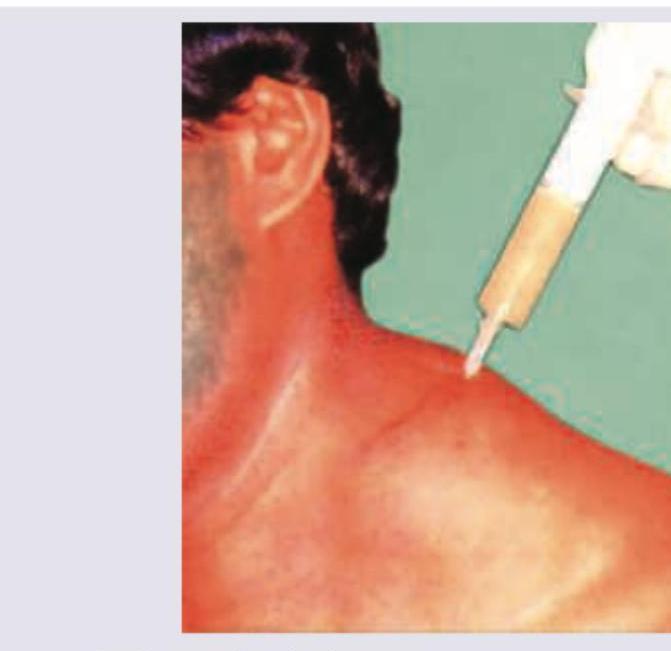
A patient presents with a cervical swelling that is fluctuant, non-tender, and lacks overlying erythema or warmth. Diagnostic aspiration yields thick, creamy pus; Ziehl-Neelsen staining confirms acid-fast bacilli. All are true about this condition except:

All are true about the image shown except:

All are true about the image shown except:
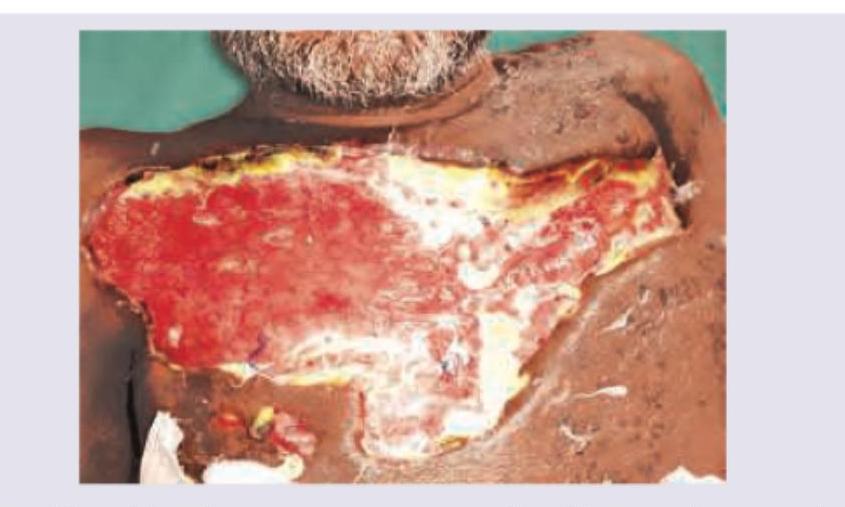
An HIV positive patient presents with symptoms of toxemia, pain out of proportion to the wound appearance, and foul smelling discharge from the lesion shown below. What is the diagnosis?
"Collar-stud" abscess is seen in :
Which of the following are risk factors for wound infection? 1. Malnutrition 2. Poor perfusion 3. Antibodies 4. Foreign body material Select the correct answer using the code given below.
The most common intraperitoneal abscess following peritonitis is
Which of the following is a scoring system for severity of wound infection, and is particularly useful for surveillance and research ?
The surgical complications of typhoid fever include all of the following except :
Practice by Chapter
Surgical Site Infections
Practice Questions
Intra-abdominal Infections
Practice Questions
Soft Tissue Infections
Practice Questions
Necrotizing Soft Tissue Infections
Practice Questions
Surgical Sepsis
Practice Questions
Tetanus Prophylaxis
Practice Questions
Antimicrobial Prophylaxis
Practice Questions
Antimicrobial Therapy in Surgical Infections
Practice Questions
Surgical Drainage Procedures
Practice Questions
Infection Control in Operating Room
Practice Questions
Biofilms and Implant-Related Infections
Practice Questions
Prevention Strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app