
Preoperative and Postoperative Care — MCQs

On this page
A 65-year-old man undergoes a technically difficult abdominoperineal resection for a rectal cancer during which he receives three units of packed red blood cells. Four hours later in the intensive care unit he is bleeding heavily from his perineal wound. Emergency coagulation studies reveal normal prothrombin, partial thromboplastin, and bleeding times. The fibrin degradation products are not elevated but the serum fibrinogen content is depressed and the platelet count is 70,000/mL. What is the most likely cause of the bleeding?
Following splenectomy in children, which one of the following is recommended?
When should antibiotics be given for surgical prophylaxis?
A 42-year-old man has had a rocky course for the 3 days following a bowel resection for intestinal perforation due to inflammatory bowel disease. His central venous pressure (CVP) had been 12 to 14 but is now 6, in the face of diminished blood pressure and oliguria. Which of the following is the most likely etiology of his hypotension?
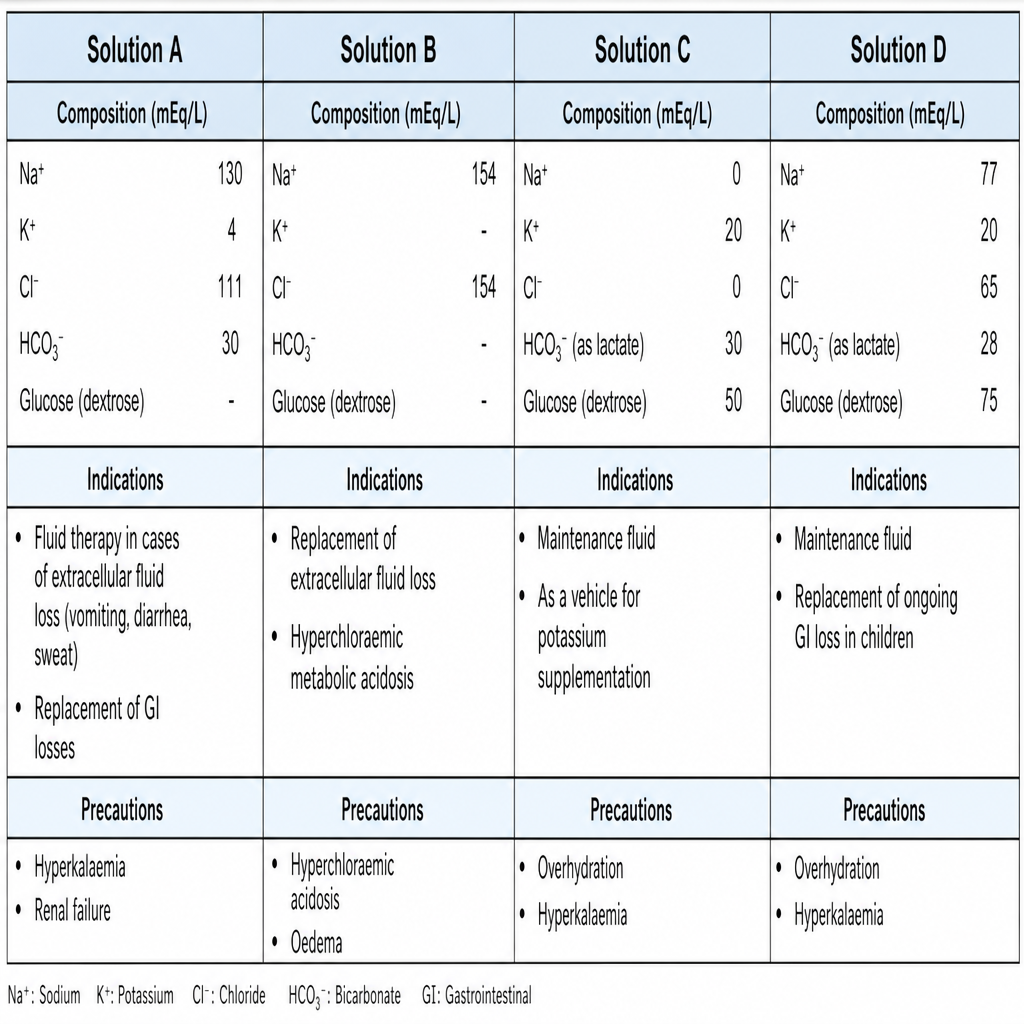
A 70-year-old woman has a small-bowel fistula with an output of 1.5 L/d. Replacement of daily losses should be handled using which of the following fluid solutions based on its composition in mEq/L?
What is the first sign of burst abdomen?
A 68-year-old hypertensive man undergoes successful repair of a ruptured abdominal aortic aneurysm. He receives 9 L Ringer's lactate solution and 4 units of whole blood during the operation. Two hours after transfer to the surgical intensive care unit, the following hemodynamic parameters are obtained: systemic blood pressure (BP) 90/60 mm Hg, pulse 110 beats per minute, central venous pressure (CVP) 7 mm Hg, pulmonary artery pressure 28/10 mm Hg, pulmonary capillary wedge pressure (PCWP) 8 mm Hg, cardiac output 1.9 L/min, systemic vascular resistance 1400 (dyne*s)/cm5 (normal is 900-1300), PaO2 140 mm Hg (FiO2: 0.45), urine output 15 mL/h (specific gravity: 1.029), and hematocrit 35%. Given this data, which of the following is the most appropriate next step in management?
Which of the following is NOT true about the principal hormonal responses to surgical stress?
A 59-year-old man is planning to undergo coronary artery bypass surgery. He has osteoarthritis and consumes nonsteroidal anti-inflammatory drugs (NSAIDs) for the pain. Which of the following is the most appropriate treatment prior to surgery to minimize his risk of bleeding from his NSAID use?
A 65-year-old man is being evaluated for possible right pneumonectomy for bronchogenic carcinoma. Which value is most suggestive of postoperative problems?
Practice by Chapter
Preoperative Risk Assessment
Practice Questions
Perioperative Management of Comorbidities
Practice Questions
Preparation of Patient for Surgery
Practice Questions
Informed Consent Process
Practice Questions
Post-Anesthesia Care
Practice Questions
Pain Management
Practice Questions
Wound Care and Dressings
Practice Questions
Drain Management
Practice Questions
Postoperative Complications Detection
Practice Questions
Early Ambulation and Rehabilitation
Practice Questions
Enhanced Recovery After Surgery (ERAS) Protocols
Practice Questions
Discharge Planning and Follow-up
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app