
Preoperative and Postoperative Care — MCQs

On this page
Which of the following agents is of no value in the postoperative care of a hemophilic patient?
An obese 50-year-old woman undergoes a laparoscopic cholecystectomy. In the recovery room she is found to be hypotensive and tachycardic. Her arterial blood gases reveal a pH of 7.29, partial pressure of oxygen of 60 kPa, and partial pressure of CO2 of 54 kPa. What is the most likely cause of this woman's problem?
What is the anticoagulant of choice for prophylaxis of venous thromboembolism in a patient undergoing cancer surgery?
A 35-year-old man with duodenal stump leak after partial gastrectomy is receiving central parenteral nutrition containing D25W and 4.25% amino acid solution. Which of the following is TRUE regarding essential fatty acid deficiency that can occur with hyperalimentation?
Bacterial pyogenic parotitis affecting the parotid gland is most common after which of the following conditions?
A 32-year-old female undergoes emergency laparotomy for perforation peritonitis. Which of the following is the surest sign of wound dehiscence?
Which of the following statements regarding the given image is false?

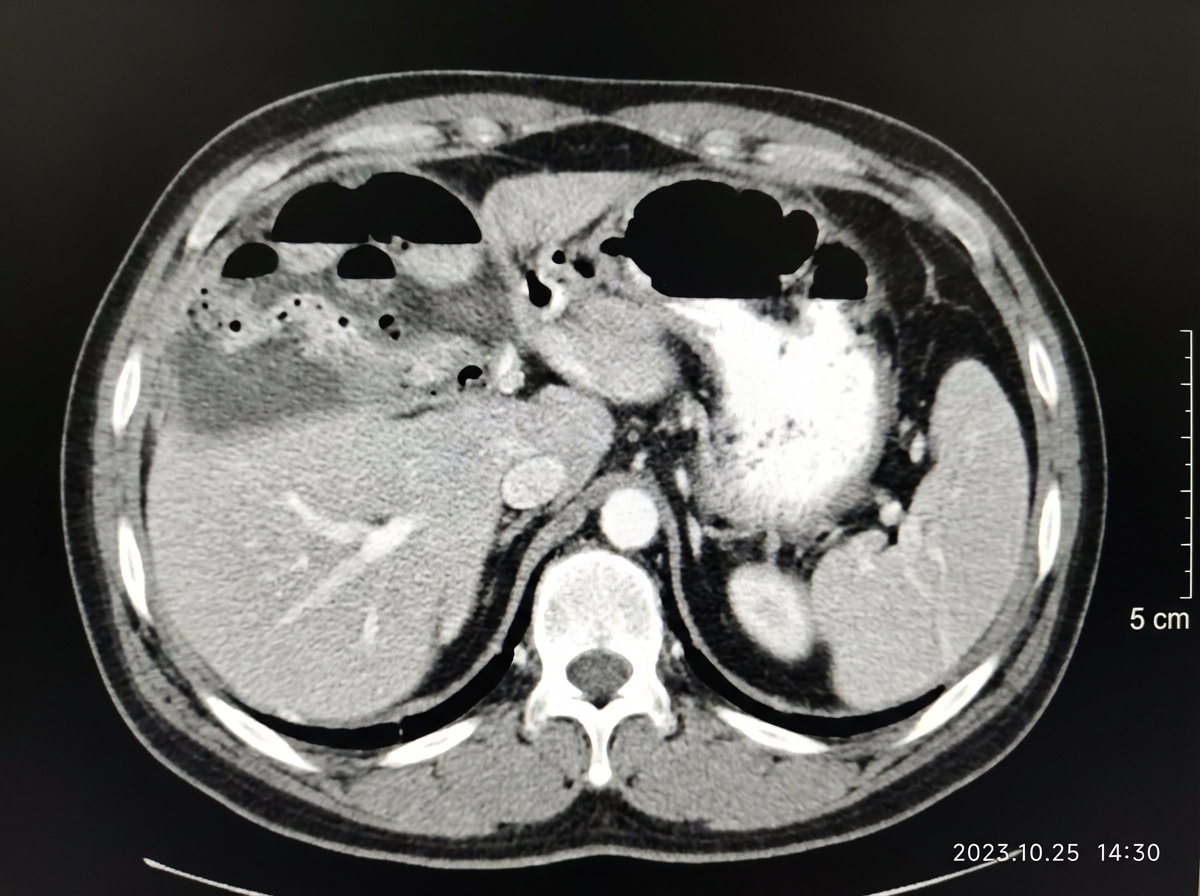
A patient after abdominal surgery presents with fever, chills, rigors along with pain in right hypochondrium, right shoulder along with Hoover's sign. Abdominal CT of the patient is given. What is the most likely diagnosis?
What does the image show? (AIIMS Nov 2018)

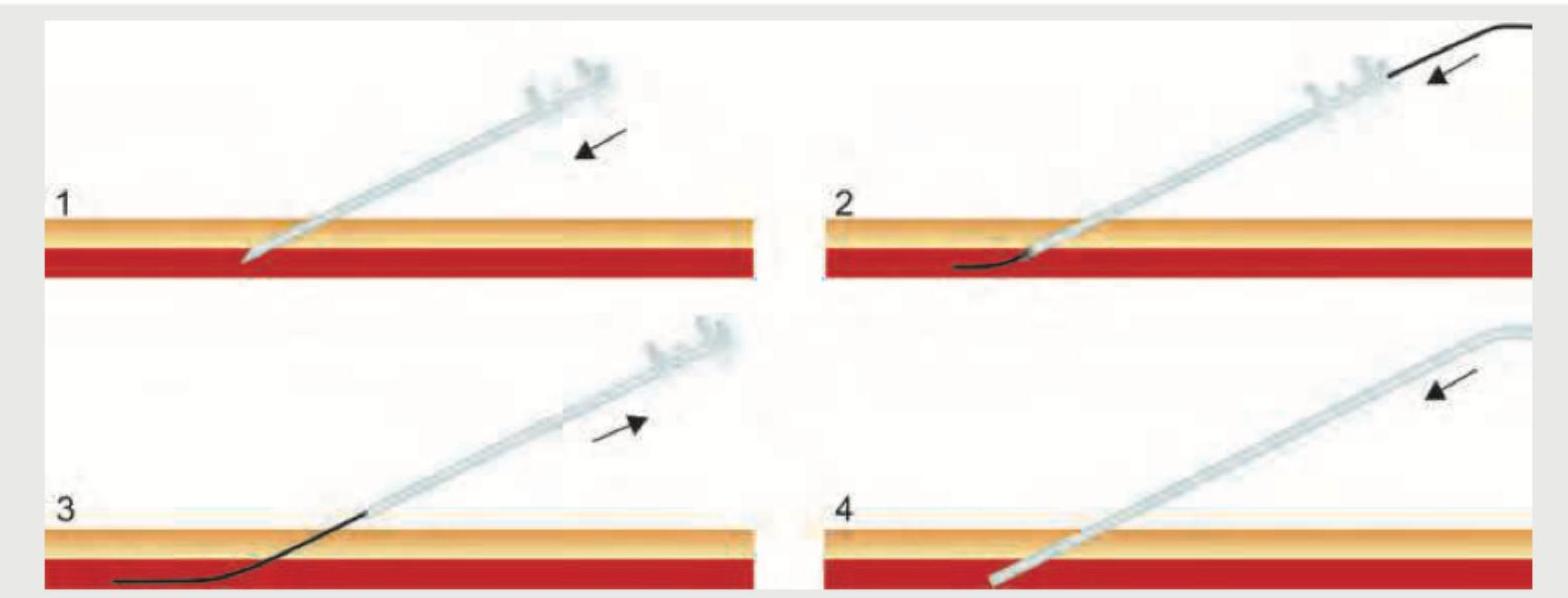
The image on the left shows a procedure. What is the procedure associated with this image?
Practice by Chapter
Preoperative Risk Assessment
Practice Questions
Perioperative Management of Comorbidities
Practice Questions
Preparation of Patient for Surgery
Practice Questions
Informed Consent Process
Practice Questions
Post-Anesthesia Care
Practice Questions
Pain Management
Practice Questions
Wound Care and Dressings
Practice Questions
Drain Management
Practice Questions
Postoperative Complications Detection
Practice Questions
Early Ambulation and Rehabilitation
Practice Questions
Enhanced Recovery After Surgery (ERAS) Protocols
Practice Questions
Discharge Planning and Follow-up
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app