
Preoperative and Postoperative Care — MCQs

On this page
What is the treatment of choice for postoperative lung collapse?
What is the primary purpose of obtaining a detailed medical history from a patient presenting for extraction?
A cirrhotic patient with abnormal coagulation studies due to hepatic synthetic dysfunction requires an urgent cholecystectomy. A transfusion of Fresh Frozen Plasma (FFP) is planned to minimize the risk of bleeding due to surgery. What is the optimal timing of this transfusion?
What is the most common site for an intra-abdominal abscess following a laparotomy?
TPN is indicated in all except?
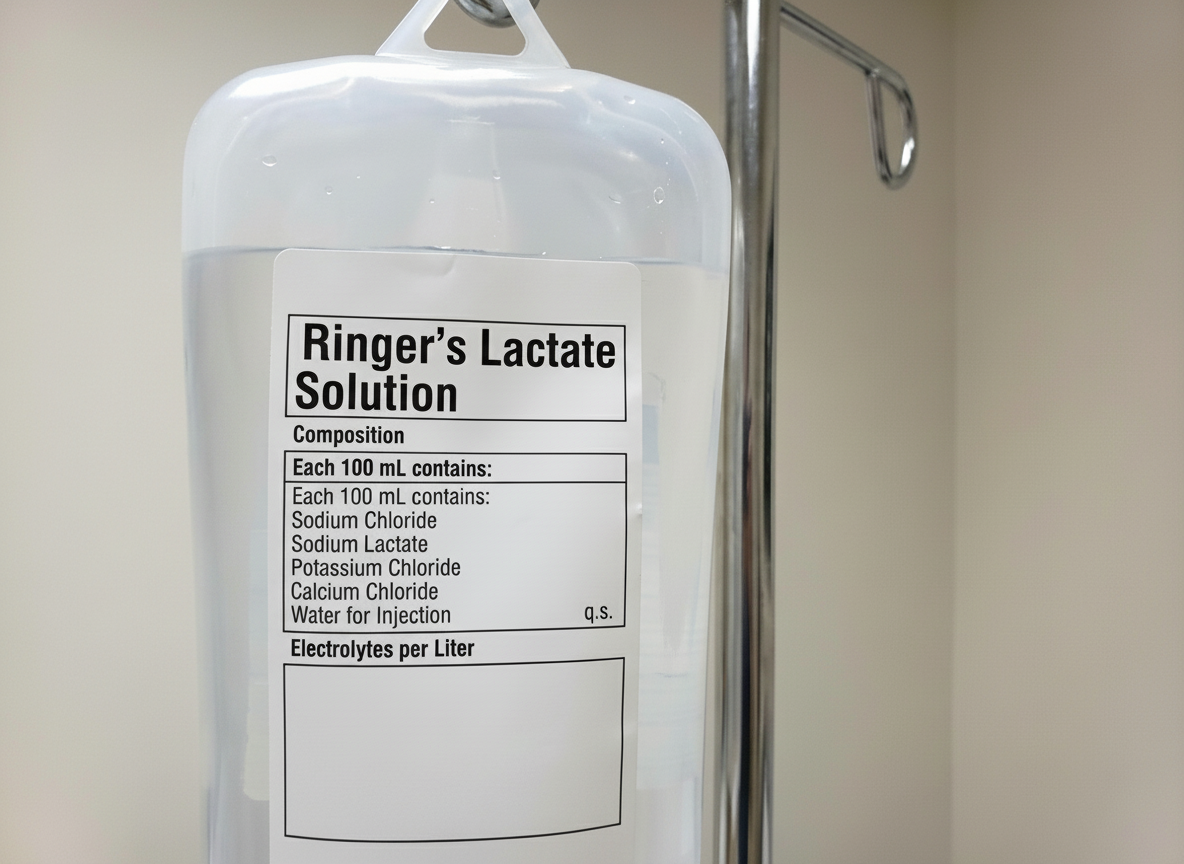
What is the total amount of potassium delivered to the patient after administering one bottle?
Prolonged postoperative ileus is best treated by?
What is the most common coagulopathy noted in surgical patients?
Which of the following are contraindications for enteral nutrition?
A 75-year-old man with a history of myocardial infarction 2 years ago, peripheral vascular disease with symptoms of claudication after walking half a block, hypertension, and diabetes presents with a large ventral hernia. He wishes to have the hernia repaired. Which of the following is the most appropriate next step in his preoperative workup?
Practice by Chapter
Preoperative Risk Assessment
Practice Questions
Perioperative Management of Comorbidities
Practice Questions
Preparation of Patient for Surgery
Practice Questions
Informed Consent Process
Practice Questions
Post-Anesthesia Care
Practice Questions
Pain Management
Practice Questions
Wound Care and Dressings
Practice Questions
Drain Management
Practice Questions
Postoperative Complications Detection
Practice Questions
Early Ambulation and Rehabilitation
Practice Questions
Enhanced Recovery After Surgery (ERAS) Protocols
Practice Questions
Discharge Planning and Follow-up
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app