
Preoperative and Postoperative Care — MCQs

On this page
What is the recommended patient positioning for Ryle's tube insertion?
A 60-year-old male underwent surgery for carcinoma of the caecum with right hemicolectomy. On the fourth postoperative day, the patient develops fever and pain in the legs. What is the most important clinical entity to suspect?
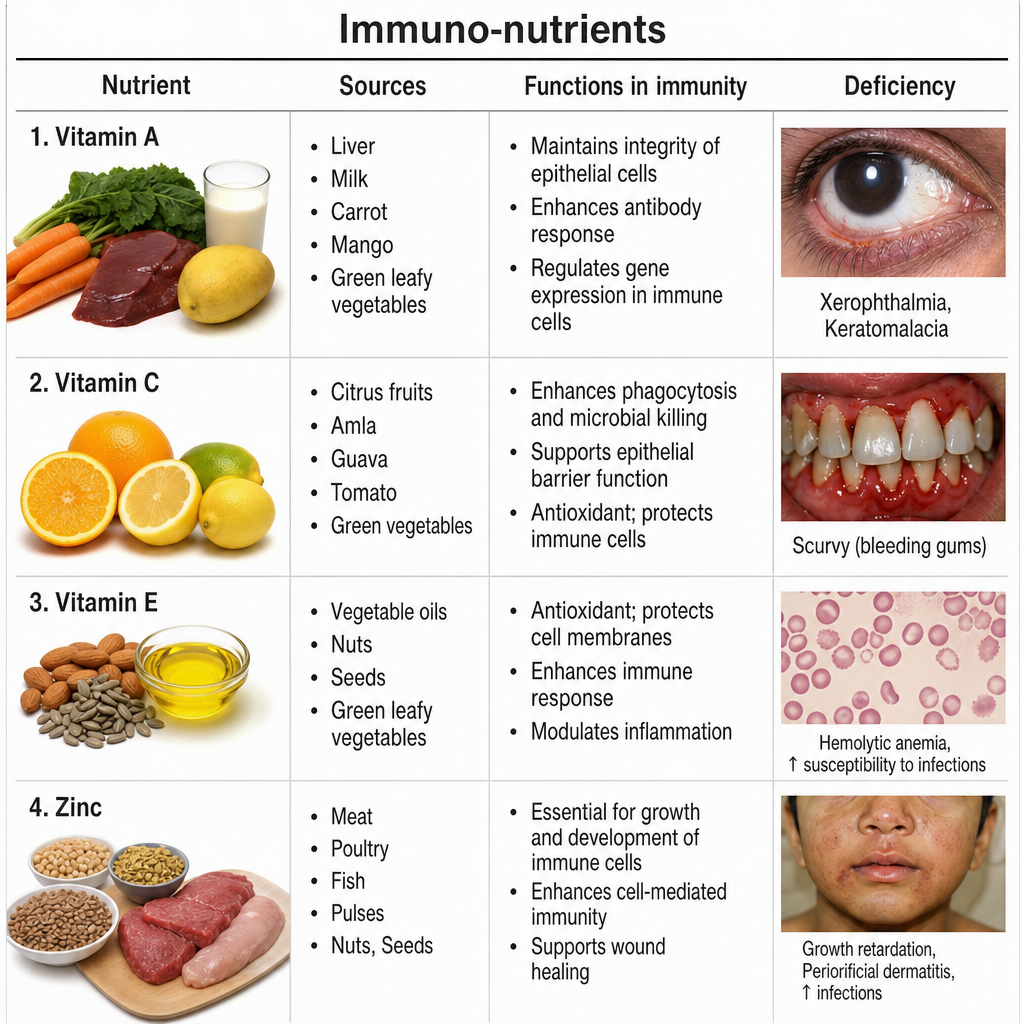
Which of the following immuno-nutrients are required more in conditions of stress? 1. Arginine 2. Glutamine 3. Omega-3 Fatty Acids 4. Nucleotides
A 40-year-old lady presents with a large left parietal convexity meningioma with perilesional edema. She is scheduled for surgery the next day. Which of the following pre-operative notes would be inappropriate to document?
In patients depending entirely on parenteral fluids, what is the expected daily weight loss?
Which of the following intravenous fluids should not be used in the first 24 hours after surgery?
Which of the following is NOT an indication for Total Parenteral Nutrition (TPN)?
In parenteral alimentation for a patient with Crohn's disease, what is the optimal ratio of calories from carbohydrates per gram of nitrogen?
In a patient receiving total parenteral nutrition, what is monitored daily?
Which is the best vein for initiating total parenteral nutrition?
Practice by Chapter
Preoperative Risk Assessment
Practice Questions
Perioperative Management of Comorbidities
Practice Questions
Preparation of Patient for Surgery
Practice Questions
Informed Consent Process
Practice Questions
Post-Anesthesia Care
Practice Questions
Pain Management
Practice Questions
Wound Care and Dressings
Practice Questions
Drain Management
Practice Questions
Postoperative Complications Detection
Practice Questions
Early Ambulation and Rehabilitation
Practice Questions
Enhanced Recovery After Surgery (ERAS) Protocols
Practice Questions
Discharge Planning and Follow-up
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app