
Preoperative and Postoperative Care — MCQs

On this page
In intravenous hyperalimentation, which of the following are administered?
A female, 12 hours post open cholecystectomy under general anesthesia, presents with dyspnea and crepitations in the right lower lobe. What is the probable cause?
In a patient recovering from peritonitis, which of the following would be the most characteristic sign of pelvic abscess?
On postoperative day 5, an otherwise healthy 55-year-old man recovering from a partial hepatectomy is noted to have a fever of 38.6°C (101.5°F). Which of the following is the most common nosocomial infection postoperatively?
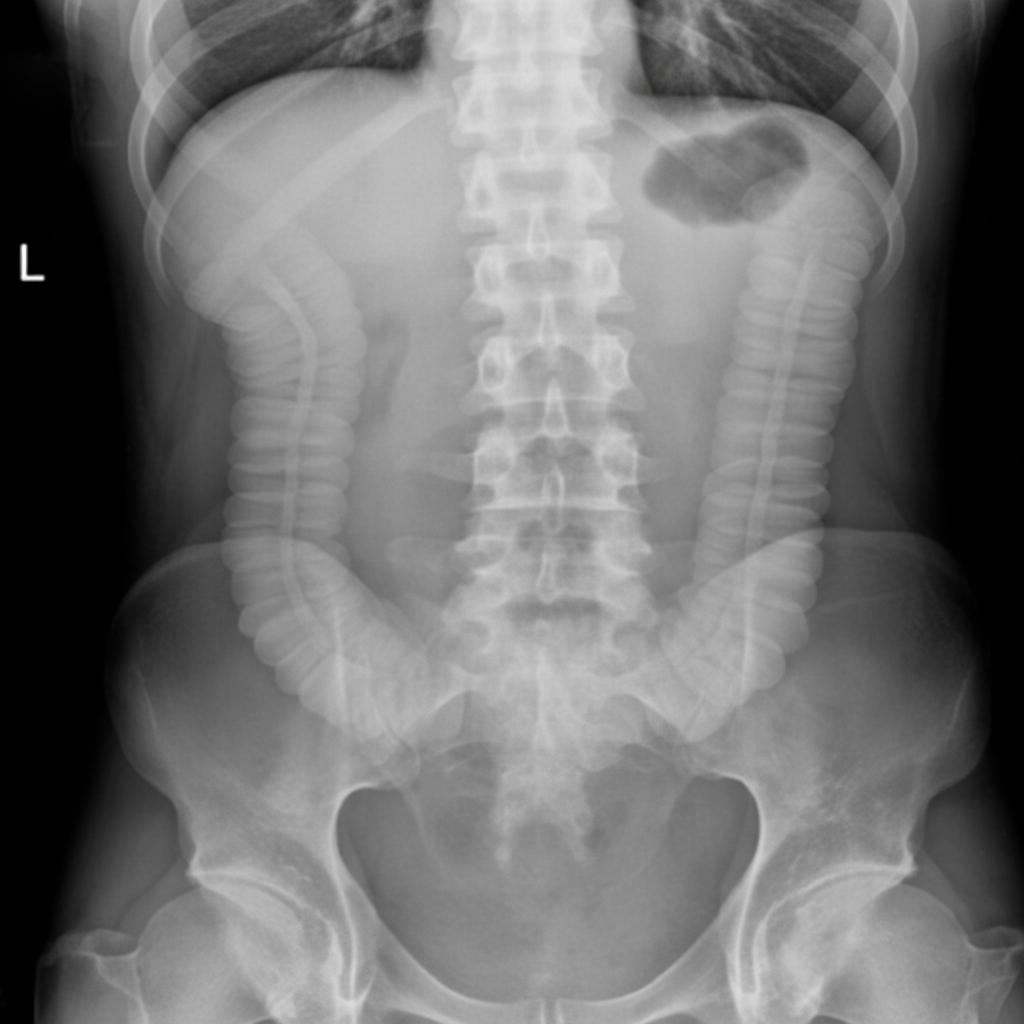
A 70-year-old woman underwent hip surgery 2 days prior for a hip fracture following a fall. She has no prior surgical history or regular medications. Over the past 24 hours, she has complained of abdominal discomfort and distension. On examination, she is afebrile with a blood pressure of 140/80 mmHg, heart rate of 110 bpm, and respiratory rate of 16 breaths/min. She has a distended, tympanic abdomen with absent bowel sounds and no rebound tenderness. Her erect abdominal X-ray is shown. What is the most likely diagnosis in this case?
A 50-year-old man with a small-bowel fistula has been receiving total parenteral nutrition (TPN) for the previous 3 weeks through a single-lumen central venous catheter. He is scheduled for exploratory laparotomy and fistula closure. On the morning of the day of surgery, TPN is discontinued and intravenous infusion with balanced salt solution (Ringer's lactate) is started. An hour later, the patient is found to be anxious, sweating, and tachycardic. What is the most likely cause?
A 60-year-old woman who underwent left hemicolectomy for diverticular disease presents with right calf pain and swelling, confirmed to be deep vein thrombosis (DVT). What is the most appropriate management?
All of the following are true about fast track surgery except?
A client who has undergone a transsphenoidal hypophysectomy should be carefully monitored for hemorrhage. Which of the following signs may indicate such bleeding?
What is the earliest sign of volume overload immediately after an operative procedure?
Practice by Chapter
Preoperative Risk Assessment
Practice Questions
Perioperative Management of Comorbidities
Practice Questions
Preparation of Patient for Surgery
Practice Questions
Informed Consent Process
Practice Questions
Post-Anesthesia Care
Practice Questions
Pain Management
Practice Questions
Wound Care and Dressings
Practice Questions
Drain Management
Practice Questions
Postoperative Complications Detection
Practice Questions
Early Ambulation and Rehabilitation
Practice Questions
Enhanced Recovery After Surgery (ERAS) Protocols
Practice Questions
Discharge Planning and Follow-up
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app