
Plastic and Reconstructive Surgery — MCQs

On this page
Best procedure for an injury to the leg with exposed bone and skin loss:
Skin grafts stored at 4°C can survive up to?
Thiersch graft consists of
Kanavel's sign is diagnosed in
Kraissl's lines are:
The best skin graft for open wounds is -
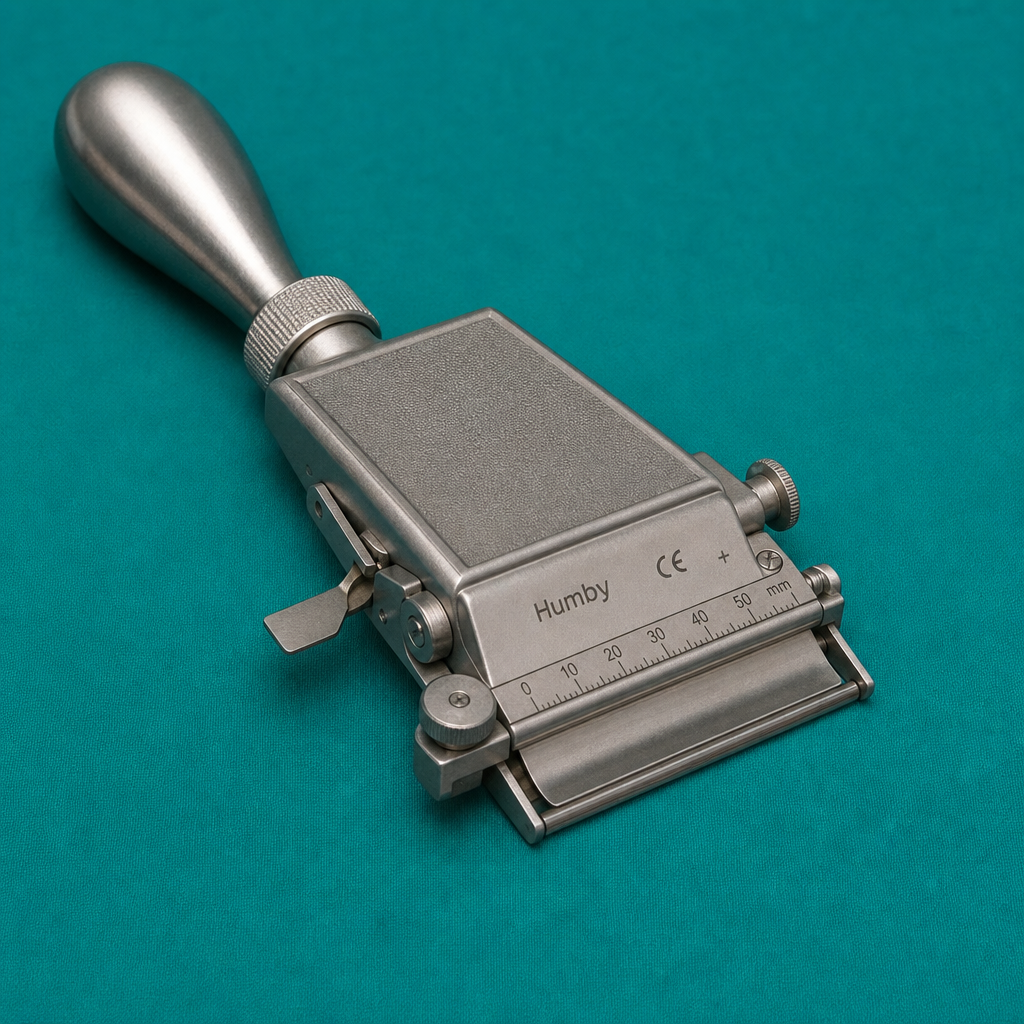
The given instrument is used for harvesting the graft from a healthy area in split-thickness skin graft. What is this called?
A Young Male complained of intermittent pain, swelling and discharge at the base of spine. He also had episodes of fever and repeated abscesses that had burst spontaneously. By occupation, he is a jeep driver. Physical examination showed pilonidal sinus. Which flap-based procedure is used for pilonidal sinus surgery?
Which type of skin graft is most appropriate for covering large full-thickness burn wounds?
In Kernahan's striped 'Y' classification, what is the main reference point?
Practice by Chapter
Wound Healing
Practice Questions
Skin Grafts
Practice Questions
Flap Surgery Principles
Practice Questions
Local Flaps
Practice Questions
Regional Flaps
Practice Questions
Microsurgical Techniques
Practice Questions
Tissue Expansion
Practice Questions
Breast Reconstruction
Practice Questions
Hand Surgery Basics
Practice Questions
Craniofacial Surgery Principles
Practice Questions
Aesthetic Surgery Concepts
Practice Questions
Body Contouring
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app