
Plastic and Reconstructive Surgery — MCQs

On this page
The best cure rates for keloids are achieved by:
Optimum age for surgery for a child with cleft lip is:
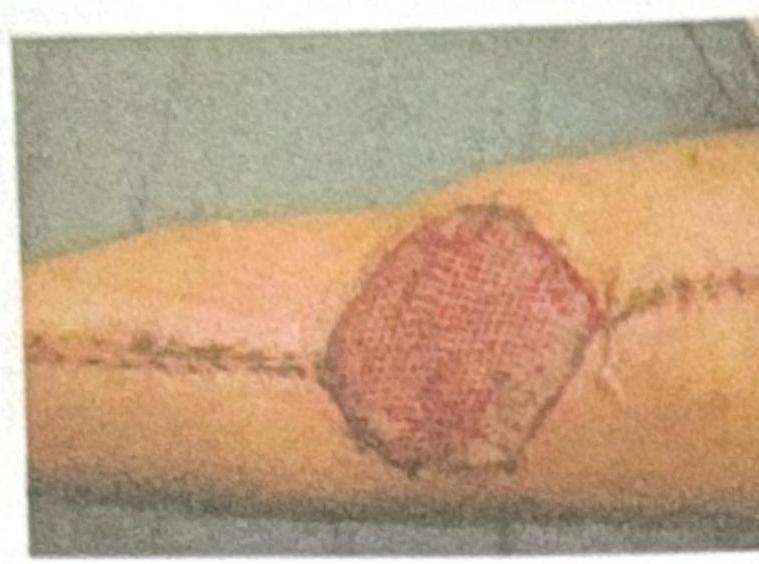
Which of the following statements about mesh skin grafts is not correct?
In Split thickness graft, which part of the skin is/are included?
Which of the following is NOT true about Dupuytren's Contracture?
How does a skin graft receive nutrition on day 3 after transplantation?
What type of graft or dressing is used to cover the post-burn wound shown in the image?
During reconstruction of an amputated limb which of the following is done first?
When osseous defects amenable to reconstruction are present, technique of choice is?
In case of burns, which graft is better for acute wound coverage?
Practice by Chapter
Wound Healing
Practice Questions
Skin Grafts
Practice Questions
Flap Surgery Principles
Practice Questions
Local Flaps
Practice Questions
Regional Flaps
Practice Questions
Microsurgical Techniques
Practice Questions
Tissue Expansion
Practice Questions
Breast Reconstruction
Practice Questions
Hand Surgery Basics
Practice Questions
Craniofacial Surgery Principles
Practice Questions
Aesthetic Surgery Concepts
Practice Questions
Body Contouring
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app