
Plastic and Reconstructive Surgery — MCQs

On this page
A patient underwent split-thickness skin grafting for a burn injury on the arm. On post-operative day 6, he develops stiffness of the arm during physiotherapy. What is the most appropriate next step in management?
A patient was brought to the emergency department following a road traffic accident. Skin grafting was done wherein the graft was taken from the same person. Which type of graft is it?
Cleft lip primary muscle repair is required in which of the following muscles?
Identify the procedure shown in the image.
What is a true statement about Z plasty?
A patient presents with an ulcer at the site of a previous burn site. All are true about the lesion except:
The following instrument used in split skin grafting is called: (Recent NEET Pattern 2016-17)

The following instrument used in split skin grafting is called: (Recent NEET Pattern 2016-17)
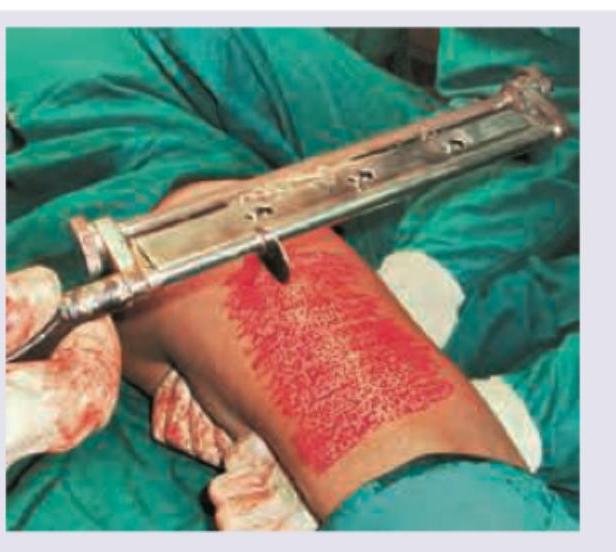
Identify this instrument which is used for harvesting graft from a healthy area in split skin grafting:

A Wolfe graft is a
Practice by Chapter
Wound Healing
Practice Questions
Skin Grafts
Practice Questions
Flap Surgery Principles
Practice Questions
Local Flaps
Practice Questions
Regional Flaps
Practice Questions
Microsurgical Techniques
Practice Questions
Tissue Expansion
Practice Questions
Breast Reconstruction
Practice Questions
Hand Surgery Basics
Practice Questions
Craniofacial Surgery Principles
Practice Questions
Aesthetic Surgery Concepts
Practice Questions
Body Contouring
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app