
Plastic and Reconstructive Surgery — MCQs

On this page
A 3.3 kg, 36-week baby girl was born prematurely after labor caused by ruptured membranes. Prenatal ultrasound revealed polyhydramnios at 26 weeks. Fetal echocardiogram was normal and amniocentesis was without genetic aberrance. On examination, there was a normal anus, and a nasogastric tube drained bile-stained fluid. The baby passed some mucus but no typical dark meconium. A chest and abdominal X-ray showed a "double bubble sign". What is the most likely diagnosis?
Which of the following statements regarding an axial flap is true?
What is the most important reason for placing an alveolar bone graft in a cleft palate patient?
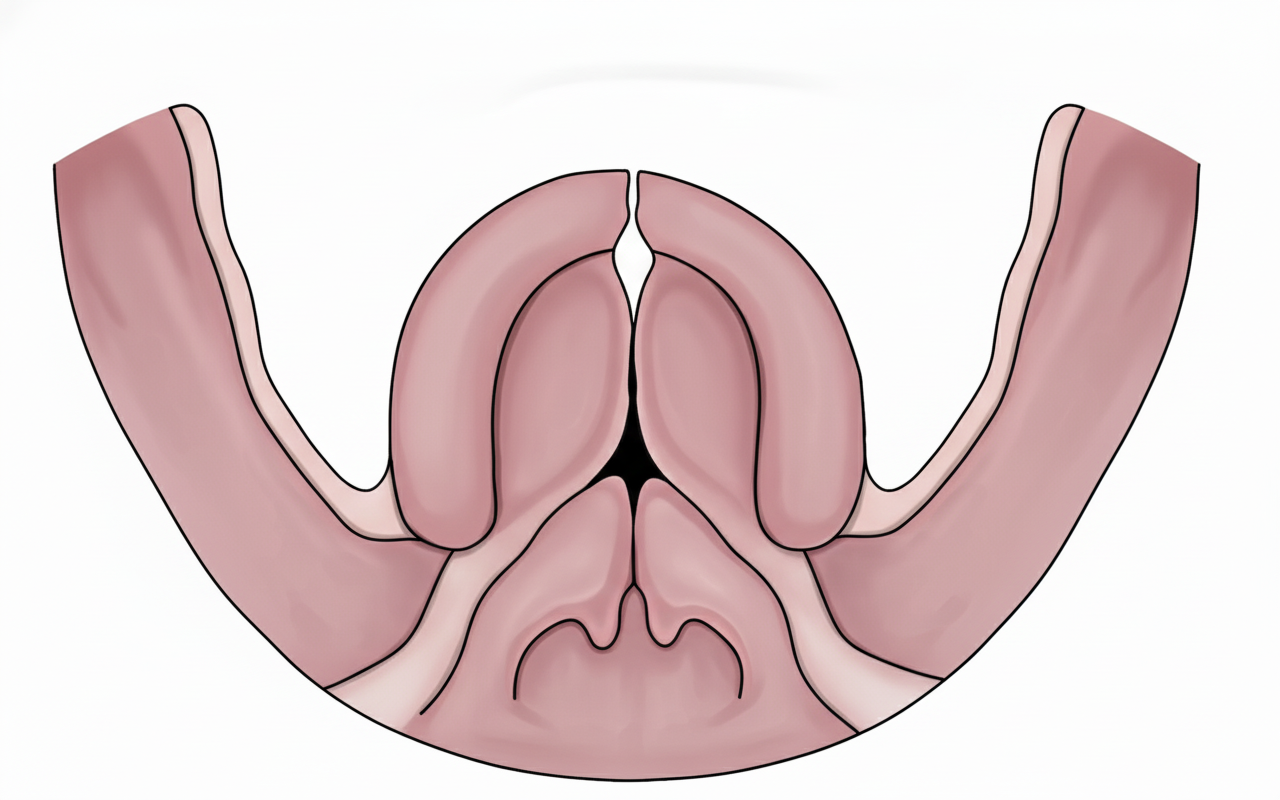
According to Veau's classification, which class does the diagrammatic representation of cleft palate belong to?
Acanthosis nigricans is typically associated with which of the following conditions?
What is the recommended incision for a felon?
What is the most important prognostic factor in melanoma?
What is Zadek's procedure?
A full thickness loss of the middle one third of the upper lip is best reconstructed by which method?
What is the most preferable graft for mandibular reconstruction?
Practice by Chapter
Wound Healing
Practice Questions
Skin Grafts
Practice Questions
Flap Surgery Principles
Practice Questions
Local Flaps
Practice Questions
Regional Flaps
Practice Questions
Microsurgical Techniques
Practice Questions
Tissue Expansion
Practice Questions
Breast Reconstruction
Practice Questions
Hand Surgery Basics
Practice Questions
Craniofacial Surgery Principles
Practice Questions
Aesthetic Surgery Concepts
Practice Questions
Body Contouring
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app