
Plastic and Reconstructive Surgery — MCQs

On this page
The rectus abdominis free flap is supplied by which artery?
Thompson's Operation for Lymphoedema is:
What is the ideal graft for a leg injury with a 10 x 10 cm exposed bone area?
Down fracture of the zygomatic arch is a treatment modality for which condition?
Which neuromuscular preserving flap is used in lip reconstruction?
The names Manchot, Salmon, and Taylor are related to which of the following?
What is the most likely diagnosis?

A free skin graft is typically rejected when transplanted onto which of the following tissues?
The Abbe estender flap is based on which artery?
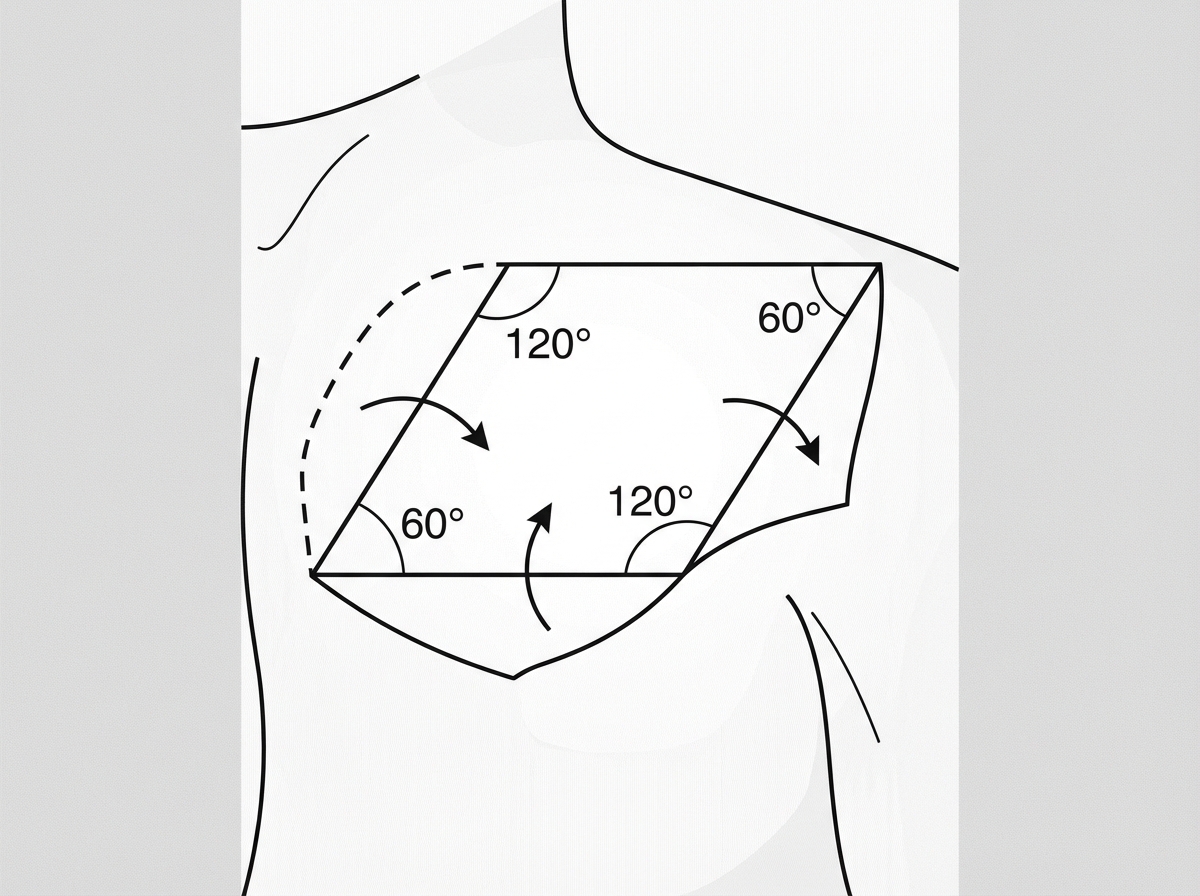
What is the name of the flap shown in the image?
Practice by Chapter
Wound Healing
Practice Questions
Skin Grafts
Practice Questions
Flap Surgery Principles
Practice Questions
Local Flaps
Practice Questions
Regional Flaps
Practice Questions
Microsurgical Techniques
Practice Questions
Tissue Expansion
Practice Questions
Breast Reconstruction
Practice Questions
Hand Surgery Basics
Practice Questions
Craniofacial Surgery Principles
Practice Questions
Aesthetic Surgery Concepts
Practice Questions
Body Contouring
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app