
Pediatric Surgery — MCQs

On this page
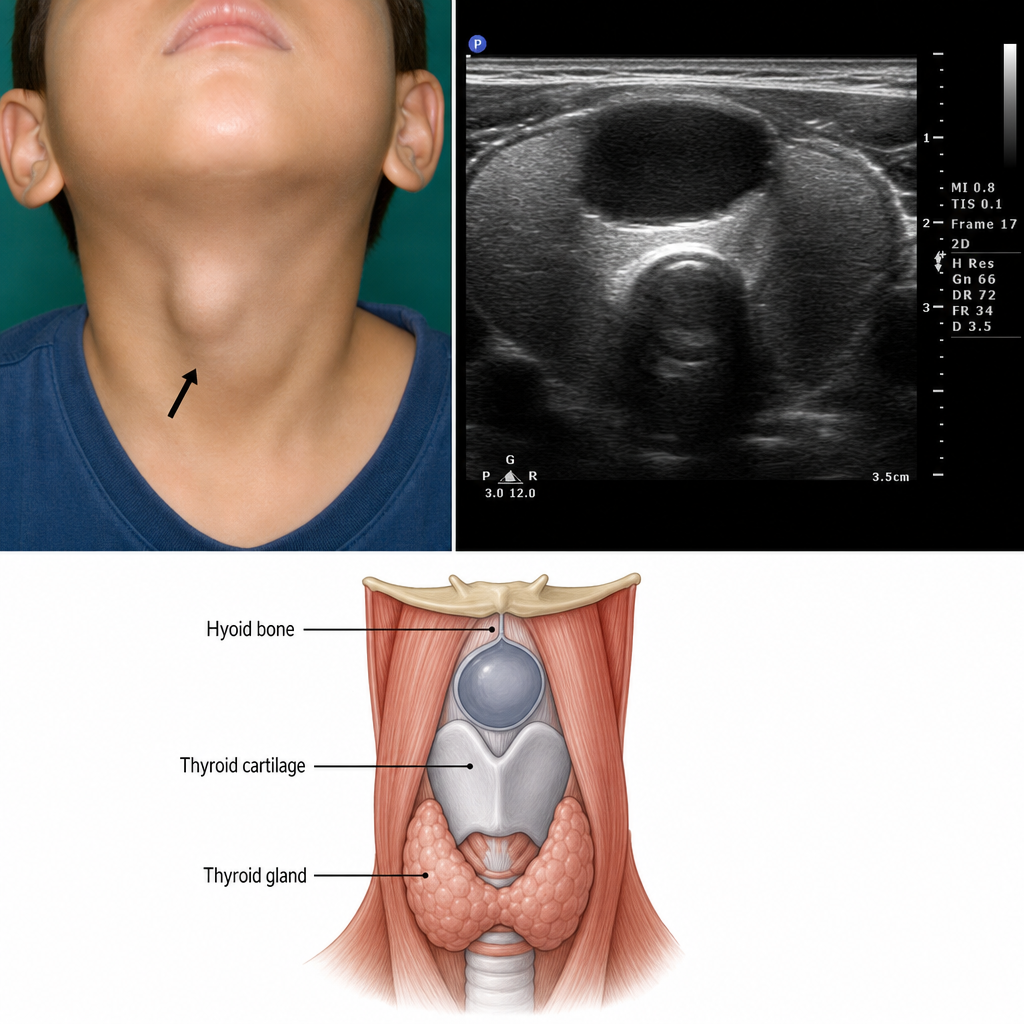
A 5-year-old boy is taken to his pediatrician for a laceration on his right knee. A mass on his neck is noticed; his mother states it has been there for several months and is slowly getting larger. The mass is slightly to the left of midline. What is the most likely diagnosis? Ultrasound of neck shows a midline hypoechoic mass anterior and superior to the thyroid gland.
The metabolic derangement in congenital pyloric stenosis is -
All of the following are true about congenital hypertrophic pyloric stenosis except
Metabolic abnormalities associated with Congenital Pyloric Stenosis in the early phase include all EXCEPT:
A child presented with intermittent episodes of left sided flank pain. Ultrasonography reveals large hydronephrosis with dilated renal pelvis and cortical thinning with a normal ureter. Kidney differential function was observed to be 19%. Which of the following is the best management?
Earliest tumour to appear after birth is?
What is the definitive treatment for Tetralogy of Fallot (TOF)?
A one-month-old female child has a swelling over the back in the sacral region. There is no cough impulse in the swelling. X-ray examination shows erosion of the coccyx. The most likely clinical diagnosis would be -
All are features of congenital megacolon except:
Congenital megacolon is confirmed by:
Practice by Chapter
Neonatal Physiology
Practice Questions
Congenital Anomalies Overview
Practice Questions
Neonatal Intestinal Obstruction
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Hirschsprung's Disease
Practice Questions
Anorectal Malformations
Practice Questions
Pediatric Hernias
Practice Questions
Pyloric Stenosis
Practice Questions
Biliary Atresia
Practice Questions
Pediatric Tumors
Practice Questions
Congenital Diaphragmatic Hernia
Practice Questions
Pediatric Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app