
Pediatric Surgery — MCQs

On this page
Which one of the following parts of intussusception is most susceptible to ischaemia and perforation?
A 16-year-old boy presents with acute onset of severe abdominal pain that began while playing basketball. He has a history of undescended testis that was surgically corrected at age 8. Physical examination shows a tender mass in the left lower quadrant. What is the most likely diagnosis and underlying mechanism?
A 4-year-old boy presents with sudden onset of severe abdominal pain and vomiting. On examination, he has a palpable mass in the right upper quadrant and bloody stools. Ultrasound shows a 'target sign' in the right abdomen. What is the most likely diagnosis and appropriate initial management?
A 3-year-old child presents with congenital diaphragmatic hernia requiring repair. Preoperative echocardiogram shows severe pulmonary hypertension with suprasystemic pressures. The pediatric surgeon recommends immediate repair, while the cardiologist suggests optimizing pulmonary pressures first. Evaluate the optimal timing and approach.
What is the diagnosis based on the image shown?

A patient presents with fecal discharge from the umbilicus. What is the most likely diagnosis?
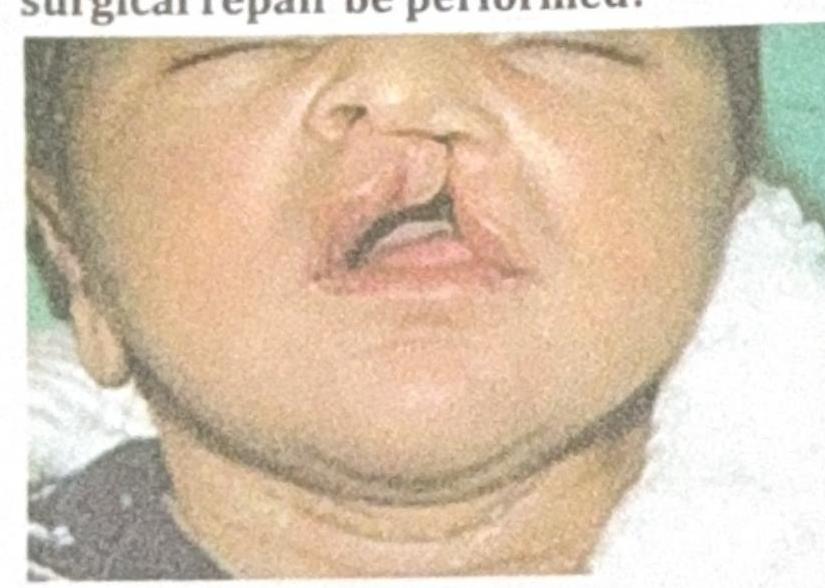
A child presents to the OPD with the finding shown in the image. When should the first surgical repair be performed?
Match the following 1. Hirschsprung's disease 2. Posterior urethral valve 3. Choledochal cyst 4. Intussusception A. Jaundice B. Currant jelly stools C. Distended abdomen D. Oligohydramnios
A 4-year-old girl is brought to the physician for a painless lump on her neck. She has no history of serious illness and her vital signs are within normal limits. On examination, there is a firm, 2-cm swelling at the midline just below the level of the hyoid bone. The mass moves cranially when she is asked to protrude her tongue. Which of the following is the most likely diagnosis?
A 6-month-old child presents with an umbilical hernia measuring 3 cm in diameter. What is the management protocol?
Practice by Chapter
Neonatal Physiology
Practice Questions
Congenital Anomalies Overview
Practice Questions
Neonatal Intestinal Obstruction
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Hirschsprung's Disease
Practice Questions
Anorectal Malformations
Practice Questions
Pediatric Hernias
Practice Questions
Pyloric Stenosis
Practice Questions
Biliary Atresia
Practice Questions
Pediatric Tumors
Practice Questions
Congenital Diaphragmatic Hernia
Practice Questions
Pediatric Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app