
Pediatric Surgery — MCQs

On this page
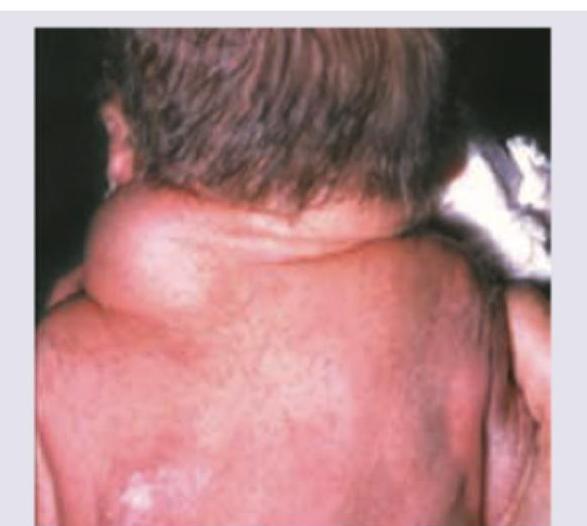
A neonate presents with a soft, compressible, translucent cystic mass in the neck region, present since birth. What is the most likely diagnosis?

A 3-year-old child presents with swelling in scrotum since birth. Transillumination test is positive. All are true except:
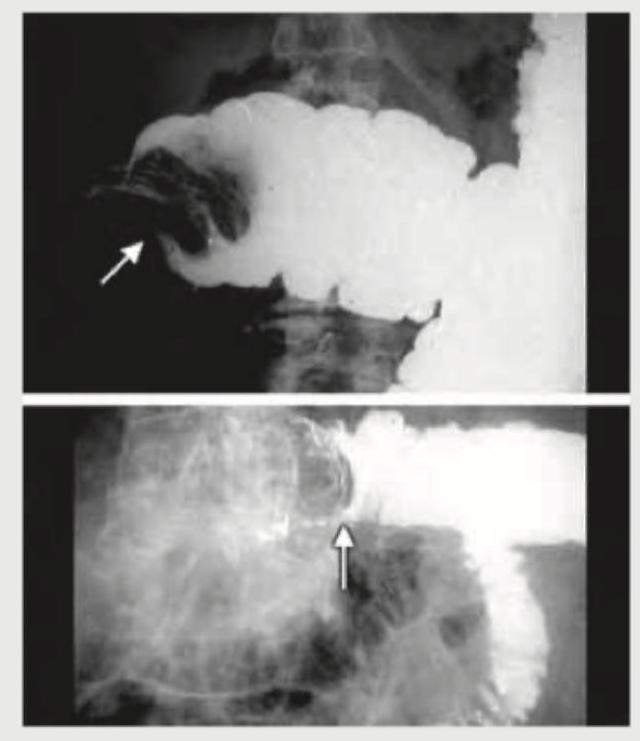
Which of the following is incorrect about the image shown?
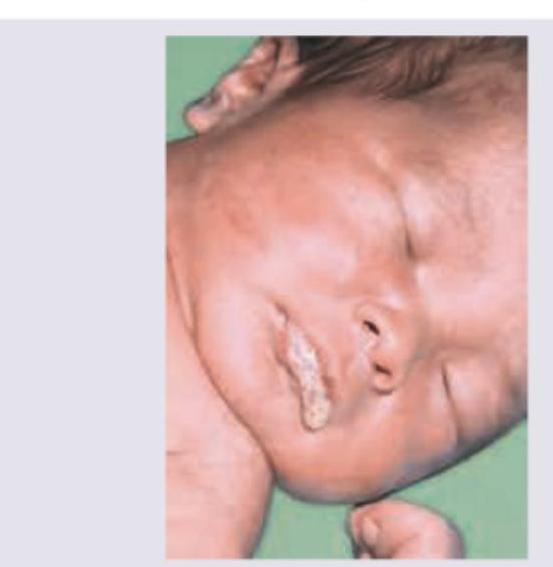
This new-born baby presented with respiratory distress soon after birth. An orogastric tube coils in the proximal pouch and abdominal gas is present on X-ray. Which of the following is not a correct association about this condition?
Identify the disease shown in the image.

All of the following statements regarding this image are true except: (Recent NEET Pattern 2016-17)
Which of the following statements are correct regarding Inguinal hernias in children? I. It is more common in premature boys. II. It should be repaired promptly. III. It is always indirect. IV. It may frequently be transilluminant. Select the answer using the code given below :
The most common site of urethral opening in cases of hypospadias is :
A 5-year-old male child comes with a left sided scrotal swelling which has no cough impulse and does not reduce on compression or lying down but the parents give a definite history that swelling is absent in the morning and comes by in the evening. The best treatment is :
Which of the following are correct for herniation via foramen of Morgagni? 1. It occurs posteriorly in chest. 2. Transverse colon is the commonest content. 3. Defect is between sternal and costal attachments. 4. It is a type of congenital hernia. Select the answer using the code given below.
Practice by Chapter
Neonatal Physiology
Practice Questions
Congenital Anomalies Overview
Practice Questions
Neonatal Intestinal Obstruction
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Hirschsprung's Disease
Practice Questions
Anorectal Malformations
Practice Questions
Pediatric Hernias
Practice Questions
Pyloric Stenosis
Practice Questions
Biliary Atresia
Practice Questions
Pediatric Tumors
Practice Questions
Congenital Diaphragmatic Hernia
Practice Questions
Pediatric Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app