
Pediatric Surgery — MCQs

On this page
The image shows:

The picture shows a newborn with esophageal atresia and distal tracheoesophageal fistula presenting with excessive salivation. Which of the following statements is NOT true regarding the condition shown?
All are true about the condition shown in the figure except:

What is shown in the image below?

A newborn male infant presents with the findings shown in the image. The clinical diagnosis is?

A 2-month-old girl was brought with swelling just above the gluteal area with progressive increase in size. Imaging reveals a midline mass attached to the coccyx with both external and internal presacral components. Which is the most probable diagnosis?

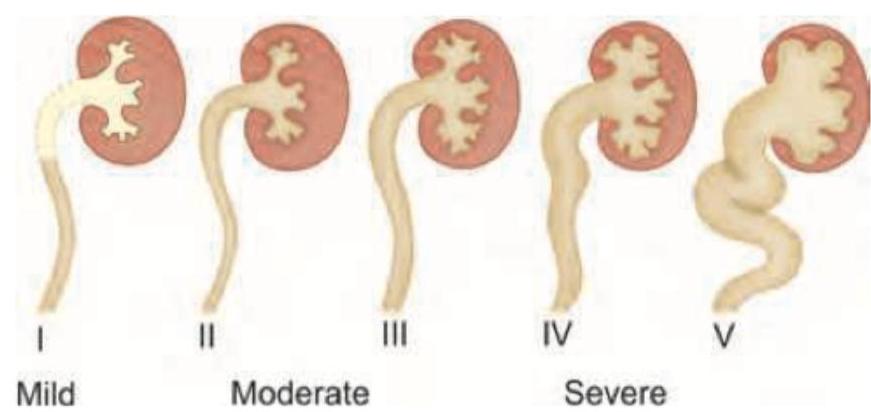
The image shows presence of:

All investigations are useful in work up of this condition except:

Which tumor is shown here?

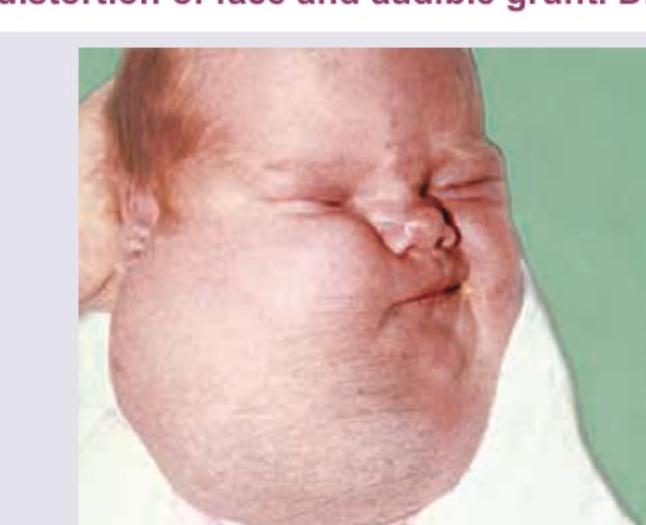
A neonate presents with a doughy soft lump in the neck causing distortion of face and audible grunt, as shown in the image. Diagnosis is:
Practice by Chapter
Neonatal Physiology
Practice Questions
Congenital Anomalies Overview
Practice Questions
Neonatal Intestinal Obstruction
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Hirschsprung's Disease
Practice Questions
Anorectal Malformations
Practice Questions
Pediatric Hernias
Practice Questions
Pyloric Stenosis
Practice Questions
Biliary Atresia
Practice Questions
Pediatric Tumors
Practice Questions
Congenital Diaphragmatic Hernia
Practice Questions
Pediatric Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app