
Pediatric Surgery — MCQs

On this page
Which of the following is true for Bochdalek hernia?
Identify the pathology in the child.
A neonate has intestines protruding from the abdomen without any external covering. What will be your next line of management?
A 2-month-old male infant presents with a scrotal swelling that has been present since birth. Now, the swelling has become suddenly painful, red, and irreducible. What is the most likely diagnosis?
Identify the type of diaphragmatic hernia shown in the X-ray.
A newborn child is brought to the emergency department with respiratory difficulty. On evaluation, the x-ray given was obtained. What is the diagnosis?
A 4-year-old boy was brought to the emergency department with complaints of melena and acute intermittent pain in the right iliac region. On surgical exploration, a diverticulum containing gastric mucosa was found. What is the diagnosis? 
A 2-month-old infant presents with projectile non-bilious vomiting after each feeding for the past week, weight loss, and constant hunger. On examination, a firm, olive-shaped mass is palpable in the right upper quadrant. Serum electrolytes show hypochloremic hypokalemic metabolic alkalosis. What is the definitive treatment?
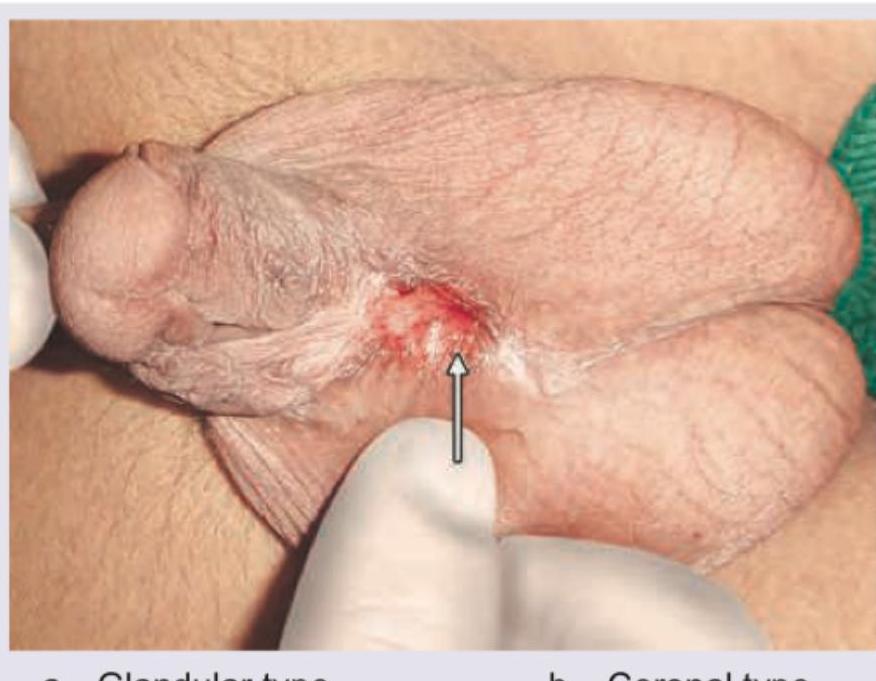
What is the malformation shown in the image?
A 28-year-old physically fit male patient presents with a condition similar to the given image, showing a 6 cm full-thickness rectal prolapse. What is the surgery of choice?

Practice by Chapter
Neonatal Physiology
Practice Questions
Congenital Anomalies Overview
Practice Questions
Neonatal Intestinal Obstruction
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Hirschsprung's Disease
Practice Questions
Anorectal Malformations
Practice Questions
Pediatric Hernias
Practice Questions
Pyloric Stenosis
Practice Questions
Biliary Atresia
Practice Questions
Pediatric Tumors
Practice Questions
Congenital Diaphragmatic Hernia
Practice Questions
Pediatric Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app