
Pediatric Surgery — MCQs

On this page
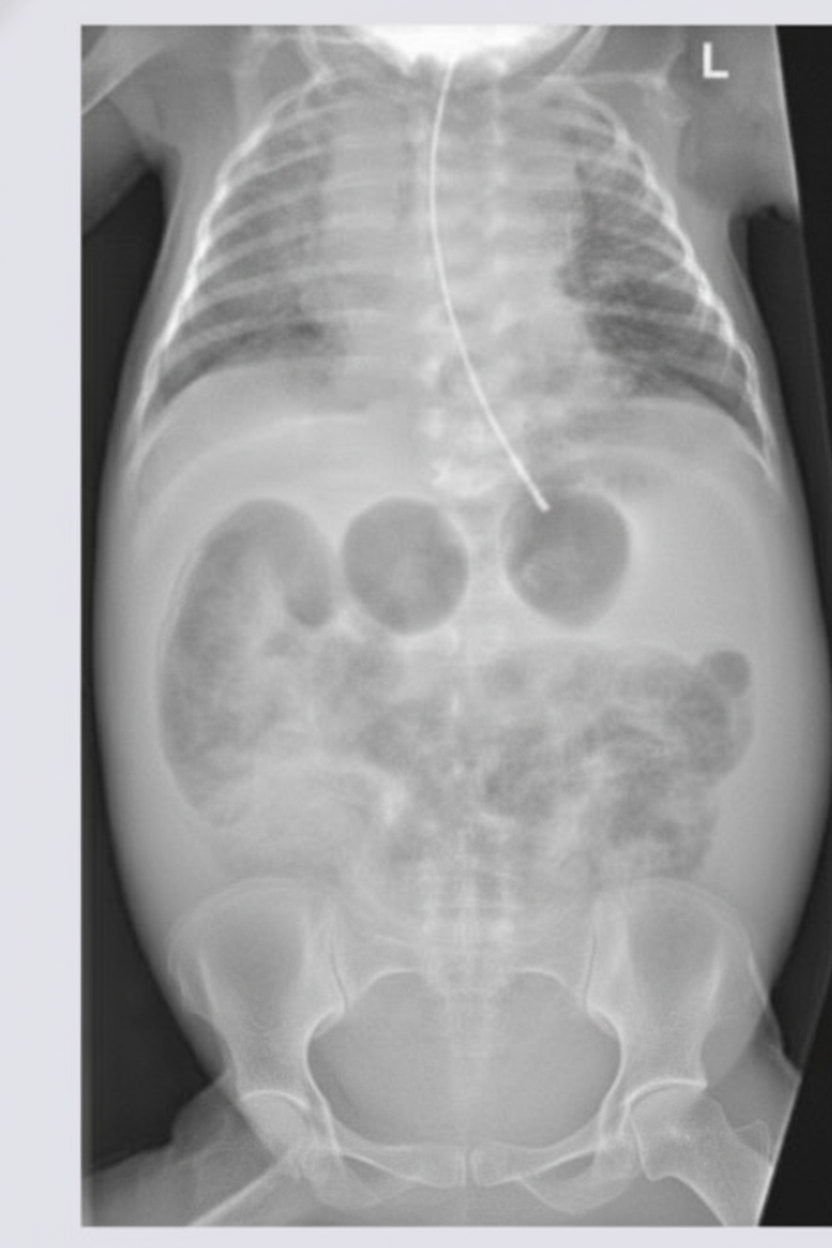
A newborn infant presents with a history of multiple episodes of bilious projectile vomiting. An X-ray of the abdomen was performed. What is the most likely diagnosis?
Which of the following statements is NOT true regarding pyloric stenosis?
What is the most common presentation of Meckel's diverticulum?
Which of the following is the treatment of choice for Stage I Wilm's Tumor?
Which of the following is NOT true about congenital hypertrophic pyloric stenosis (CHPS)?
Which of the following is a true congenital hernia through the foramen of Bochdalek?
In pyloric stenosis, the following changes are seen?
What is the commonest cause of intestinal obstruction in a newborn?
According to Moore's classification of omphalocole (examphalos), type I umbilical defect is less than what size in cm?
A 55-day-old infant born prematurely at 27 weeks of gestation presents with a non-tender, firm swelling that is not hot or red. The swelling does not transilluminate and appears to resolve with pressure but returns when the infant cries or strains. What is the most appropriate course of action?
Practice by Chapter
Neonatal Physiology
Practice Questions
Congenital Anomalies Overview
Practice Questions
Neonatal Intestinal Obstruction
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Hirschsprung's Disease
Practice Questions
Anorectal Malformations
Practice Questions
Pediatric Hernias
Practice Questions
Pyloric Stenosis
Practice Questions
Biliary Atresia
Practice Questions
Pediatric Tumors
Practice Questions
Congenital Diaphragmatic Hernia
Practice Questions
Pediatric Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app