
Pediatric Surgery — MCQs

On this page
What is the incidence of undescended testis in preterm infants?
If the mucosa is accidentally opened during a Ramstedt operation, what is the recommended duration for withholding oral feeding?
Unilateral undescended testes is ideally operated around what age?
The EXIT (Ex utero intrapartum therapy) procedure is indicated for fetal conditions that obstruct the airway or impede ventilation. In which of the following conditions is the EXIT procedure NOT indicated?
A newborn with meningomyelocele is scheduled for surgery. What should be immediately used to cover the defect?
Which type of hypospadias does not typically require surgical intervention?
Which of the following surgical techniques is not used in the management of hypospadias?
A boy with undescended testis, what is the primary concern that necessitates surgical intervention?
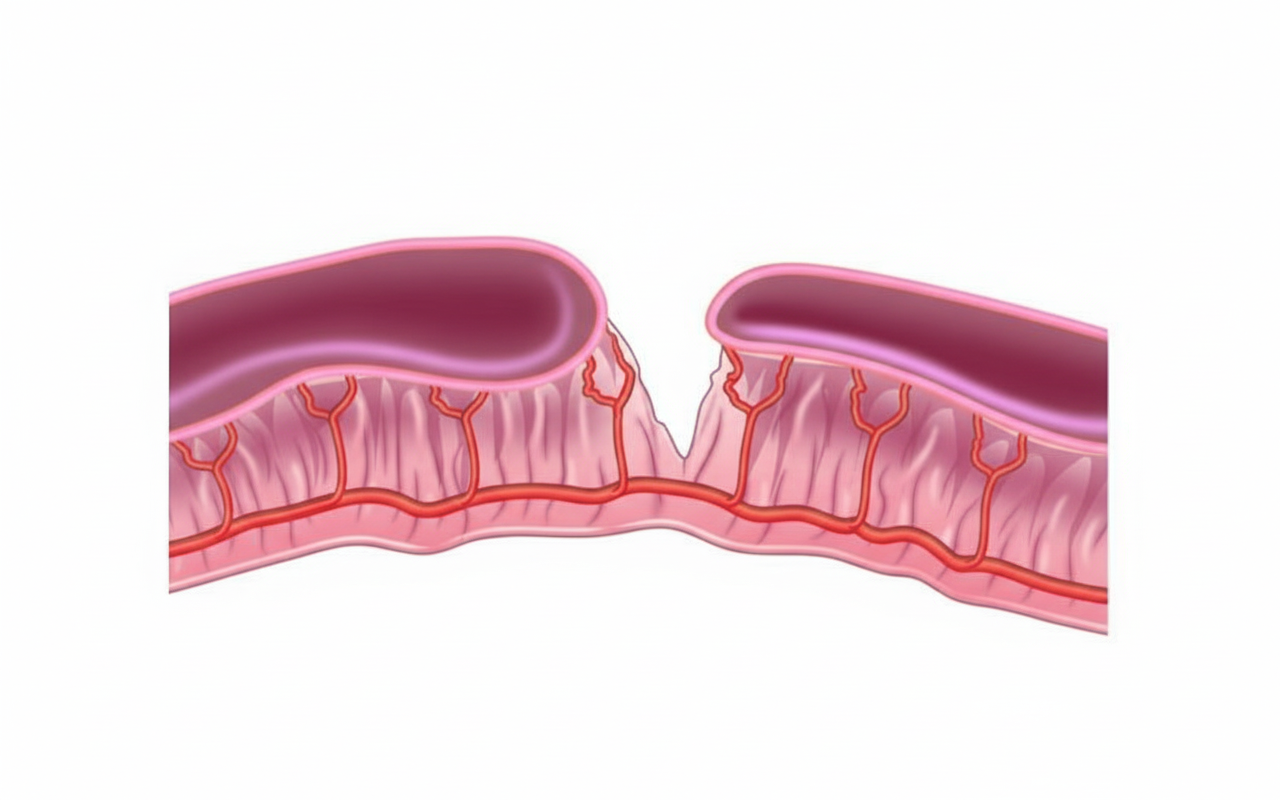
What is the type of the given intestinal atresia?
What is the most common cause of pseudopancreatic cysts in children?
Practice by Chapter
Neonatal Physiology
Practice Questions
Congenital Anomalies Overview
Practice Questions
Neonatal Intestinal Obstruction
Practice Questions
Necrotizing Enterocolitis
Practice Questions
Hirschsprung's Disease
Practice Questions
Anorectal Malformations
Practice Questions
Pediatric Hernias
Practice Questions
Pyloric Stenosis
Practice Questions
Biliary Atresia
Practice Questions
Pediatric Tumors
Practice Questions
Congenital Diaphragmatic Hernia
Practice Questions
Pediatric Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app