
Pancreatic Surgery — MCQs

On this page
A 30-year-old female with a history of chronic alcoholism presents with sudden onset of epigastric pain radiating to the back. What laboratory findings would NOT be expected in this scenario?
What is the treatment of choice for annular pancreas?
Which of the following can cause pancreatitis?
Pancreaticoduodenectomy is not indicated in which of the following conditions?
A 30-year-old patient is investigated for acute pancreatitis. Which scoring system is used for the early prediction of mortality?
Which of the following conditions is not an indication for pancreaticoduodenectomy?
A 5 cm pancreatic pseudocyst with a duration of 3 weeks should be managed by which method?
Which of the following statements regarding insulinoma is true?
What is the commonest cause of acute pancreatitis?
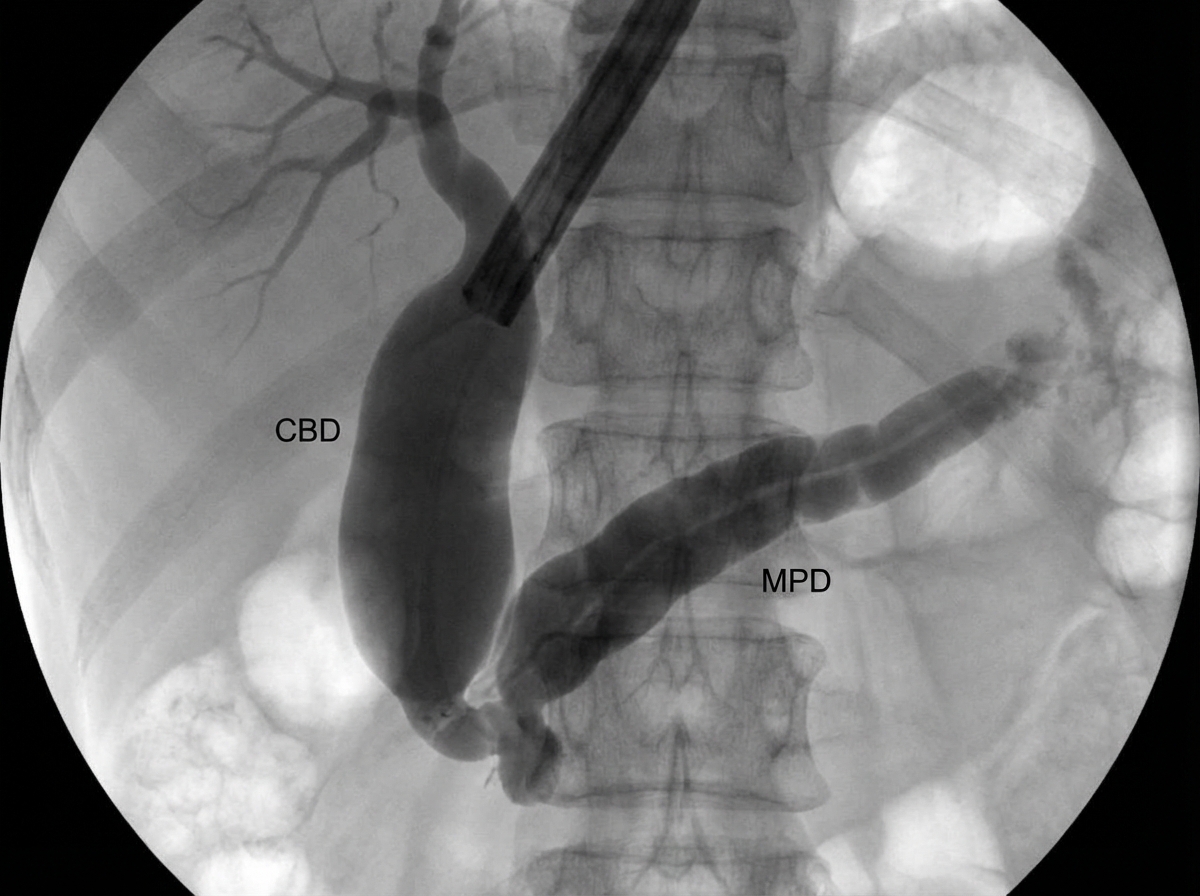
A 60-year-old chronic smoker presented with jaundice, anorexia, and weight loss. ERCP was performed. What is the most likely diagnosis based on ERCP findings?
Practice by Chapter
Pancreatic Anatomy and Physiology
Practice Questions
Acute Pancreatitis
Practice Questions
Chronic Pancreatitis
Practice Questions
Pancreatic Pseudocysts
Practice Questions
Pancreatic Adenocarcinoma
Practice Questions
Cystic Neoplasms of Pancreas
Practice Questions
Neuroendocrine Tumors of Pancreas
Practice Questions
Pancreatic Trauma
Practice Questions
Pancreatectomy Techniques
Practice Questions
Whipple Procedure
Practice Questions
Pancreatic Anastomosis
Practice Questions
Complications of Pancreatic Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app