
Pancreatic Surgery — MCQs

On this page
Which tumor is commonly seen in the area marked below?
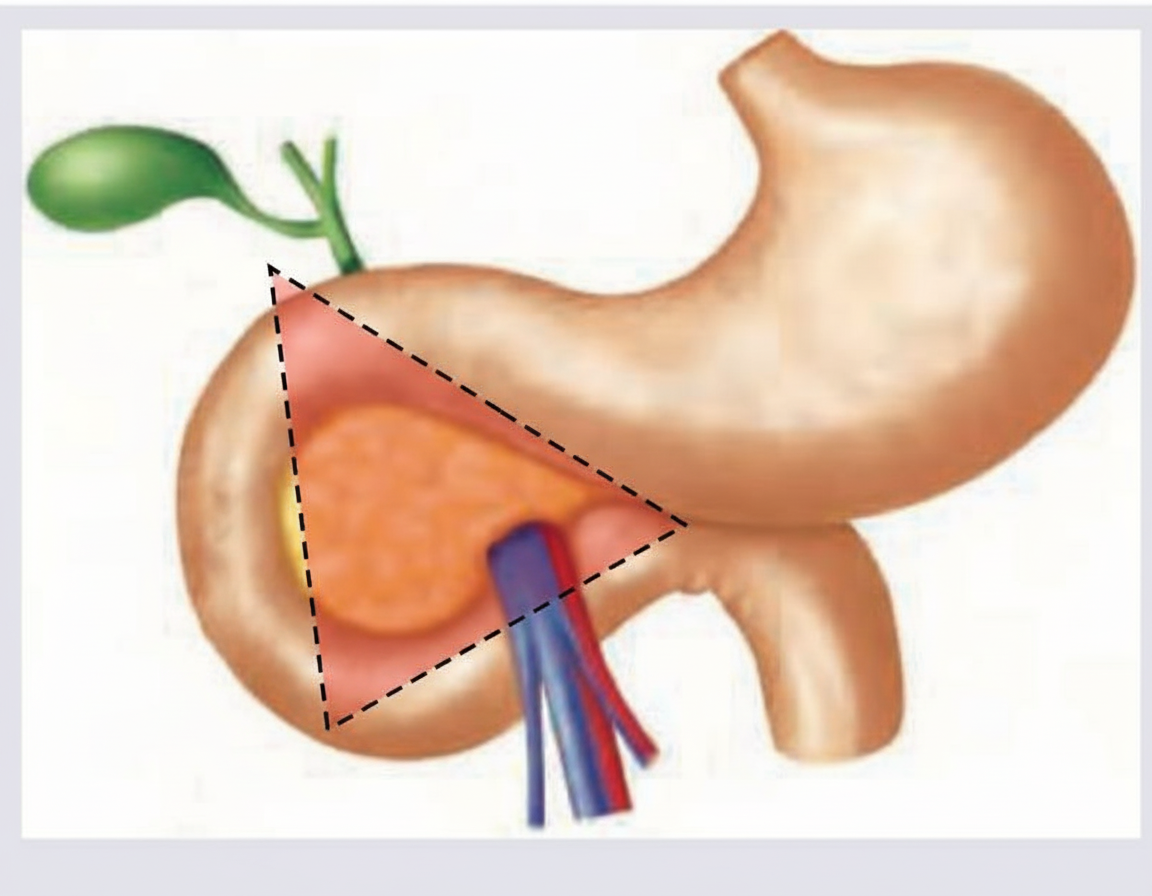
Gastrinoma is classically associated with which of the following?
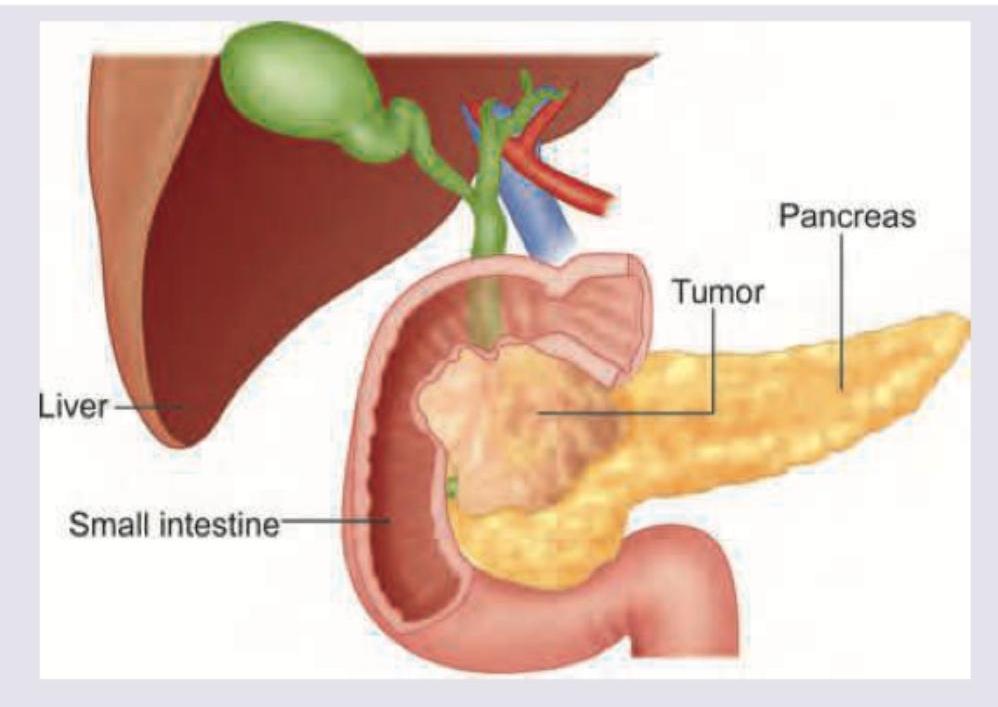
A patient with obstructive jaundice has the following imaging findings suggestive of pancreatic cancer. Which is the most appropriate method for obtaining tissue diagnosis?
Which of the following is not an indication for surgical intervention in acute pancreatitis?
A 65-year-old patient presents with obstructive jaundice and 15 kg weight loss. An ultrasound shows a 4 cm mass in the head of the pancreas with dilated bile ducts. Further work up includes a helical CT scan. The study shows several lesions consistent with metastasis in the right and left lobes of the liver and encasement of gastroduodenal artery. The most appropriate treatment would be:
In acute pancreatitis, surgery is indicated in which one of the following conditions?
A 40-year old alcoholic male complains of acute pain in the epigastrium associated with vomiting for the last 10 days. On clinical examination, he is found to have a mass in the epigastrium. The most likely diagnosis is
During Pylorus preserving pancreatico-duodenectomy (PPPD) the following organs are removed except:
A 45 year old female presented with a cystic lesion in the lesser sac on CT scan. Endoscopic ultrasound guided aspiration showed amylase to be 500 IU and carcinoembryonic antigen as 500ng/ml. What was she suffering from?
Pancreatic pseudocysts developing complications are best managed by?
Practice by Chapter
Pancreatic Anatomy and Physiology
Practice Questions
Acute Pancreatitis
Practice Questions
Chronic Pancreatitis
Practice Questions
Pancreatic Pseudocysts
Practice Questions
Pancreatic Adenocarcinoma
Practice Questions
Cystic Neoplasms of Pancreas
Practice Questions
Neuroendocrine Tumors of Pancreas
Practice Questions
Pancreatic Trauma
Practice Questions
Pancreatectomy Techniques
Practice Questions
Whipple Procedure
Practice Questions
Pancreatic Anastomosis
Practice Questions
Complications of Pancreatic Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app