
Pancreatic Surgery — MCQs

On this page
Which one of the following regarding Pancreatic effusion is correct?
Pancreatic pseudocysts developing complications are best managed by?
Treatment of choice for annular pancreas is
The following procedures are recommended for palliation in a patient with obstructive jaundice due to unresectable carcinoma of head of pancreas except:
The commonest major surgical complication following Whipple procedure is:
The most common complication of pancreas divisum is:
A 52-year-old man presents with an 8 cm pancreatic head mass with biliary obstruction. Biopsy shows adenocarcinoma. Staging shows no distant metastases, but the tumor encases the superior mesenteric artery. The oncologist recommends neoadjuvant therapy, the patient wants immediate surgery, and the family requests a second opinion. Evaluate the management approach.
A 20-year-old football player received a hard kick in the epigastrium. A large cystic swelling appeared in the epigastrium two weeks later. The most likely diagnosis is:
Carcinoma of pancreas attains largest size when it is sited in -
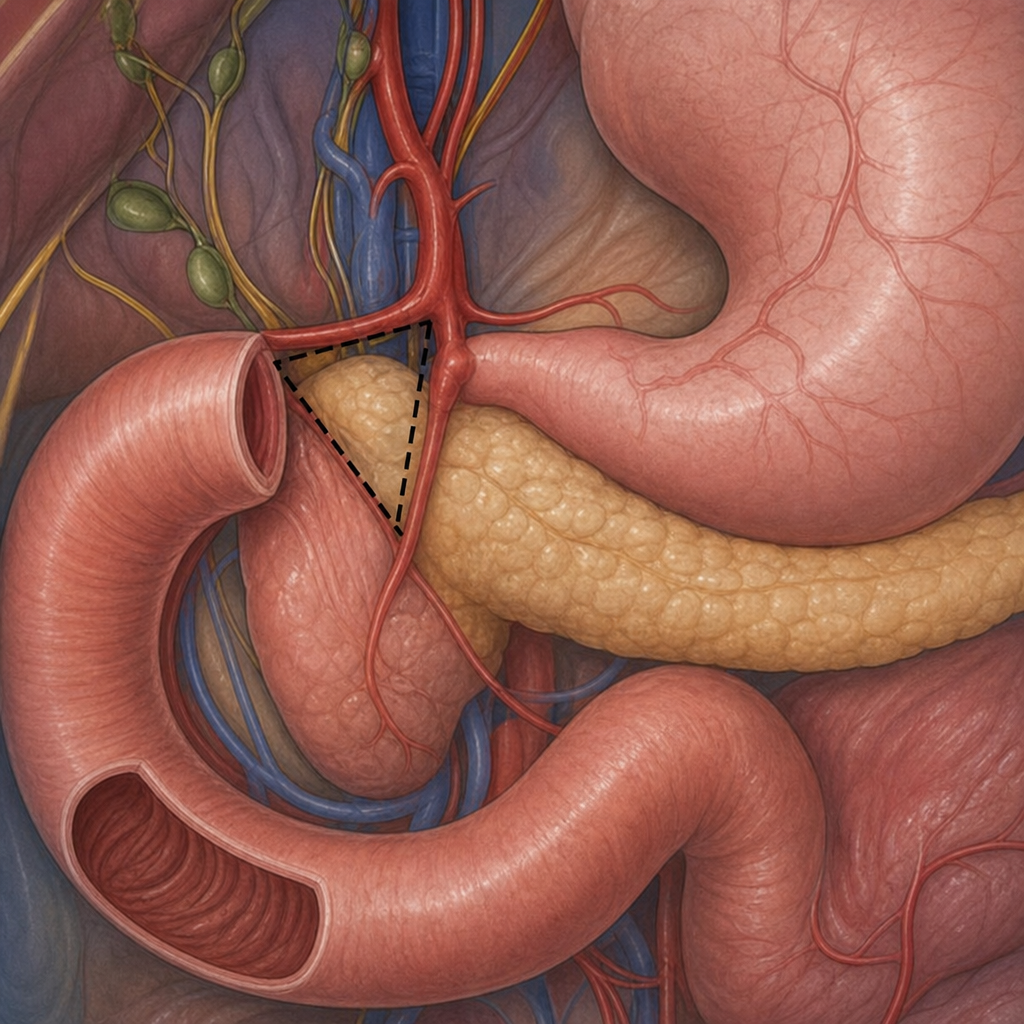
What is the name of this triangle?
Practice by Chapter
Pancreatic Anatomy and Physiology
Practice Questions
Acute Pancreatitis
Practice Questions
Chronic Pancreatitis
Practice Questions
Pancreatic Pseudocysts
Practice Questions
Pancreatic Adenocarcinoma
Practice Questions
Cystic Neoplasms of Pancreas
Practice Questions
Neuroendocrine Tumors of Pancreas
Practice Questions
Pancreatic Trauma
Practice Questions
Pancreatectomy Techniques
Practice Questions
Whipple Procedure
Practice Questions
Pancreatic Anastomosis
Practice Questions
Complications of Pancreatic Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app